
Biomarkers In Medicine: Principles, Applications, and Method Considerations
- Define the biological question and intended context of use.
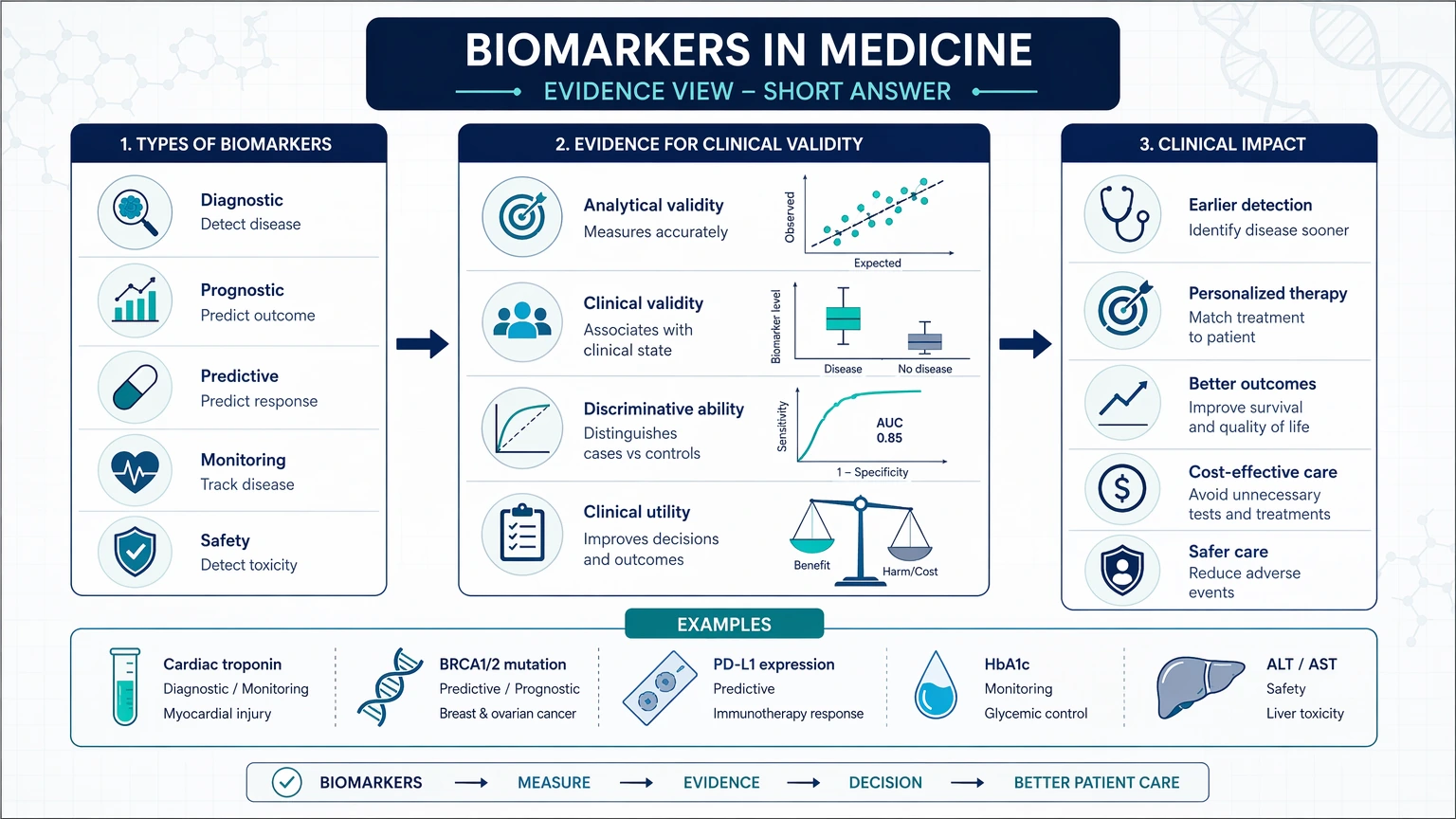
- Classify the marker by function, such as a diagnostic biomarker, prognostic biomarker, predictive biomarker, pharmacodynamic biomarker, or safety biomarker.
- Choose an assay and study design that can measure the signal with appropriate sensitivity, specificity, precision, and reproducibility in the selected specimen matrix.
- A biomarker is a measurable biological signal.
- A clinical endpoint reflects how a patient feels, functions, or survives.
- A surrogate endpoint is a biomarker intended to substitute for a clinical endpoint, which requires substantially stronger evidence than exploratory or translational biomarker use.
- Discovery identifies candidate signals.
- Verification asks whether the signal can be measured reproducibly in relevant samples.
- Validation establishes the evidence needed for the intended use, which may include fit-for-purpose validation, broader analytical validation, and eventually clinical validation.
- Define the intended use. Decide whether the marker is exploratory, translational, stratification-focused, pharmacodynamic, safety-related, or tied to another specific context of use.
- Specify the decision point. Determine whether the result will rank compounds, support dose selection, enrich a cohort, or monitor response over time.
- Choose the matrix and timepoints. Align sample type and collection schedule with the biological window of the marker.
- Match assay maturity to program stage. Early screens may need only fit-for-purpose validation, while later decision-making may require broader analytical validation.
- Plan controls and interpretation thresholds. Include suitable reference materials, negative and positive controls, and prespecified rules for outliers and below-quantitation values.
- What biological hypothesis links the biomarker to mechanism, disease state, treatment response, or safety signal?
- What is the exact context of use: diagnostic-supporting, prognostic, predictive, pharmacodynamic, safety-related, or exploratory?
- Which matrix contains the relevant molecular form, and can that sample be collected consistently at the required timepoints?
- Does the chosen method have sufficient sensitivity, specificity, precision, and dynamic range for expected concentrations?
- Which preanalytical steps are most likely to distort the signal?
- Is an orthogonal method needed to confirm analyte identity or support interpretation?
- Will longitudinal analysis require stronger controls for stability, normalization, and batch drift?
- What level of validation is justified by the intended decision?
- the biomarker class and intended decision,
- the preferred specimen matrix and collection constraints,
- whether the program needs broad discovery, targeted quantitation, or an orthogonal confirmation method,
- the expected concentration range and likely matrix effects,
- the level of method development or validation needed for the current stage.
Short Answer
For most research and drug-development programs, the right path for biomarkers in medicine starts with three linked decisions:
Before a team interprets results or expands a program, it should confirm that preanalytical variability, matrix effect, normalization strategy, dynamic range, and assay maturity all fit the decision the study is meant to support. A biomarker is not useful because the biology is interesting alone; it becomes useful when biological rationale, sample access, analytical performance, and interpretation limits are aligned.
What Are Biomarkers in Medicine?
In research and translational settings, a biomarker is a measurable characteristic that reflects a biological process, disease state, exposure, treatment response, or safety signal. Biomarkers may be molecular, cellular, histologic, physiologic, or imaging-based. A molecular biomarker can include a protein, metabolite, nucleic acid, lipid, or post-translational modification. What matters is that the marker is measurable and tied to a defined biological question.
This definition is broader than clinical decision-making. A biomarker may be useful well before it reaches clinical utility. For example, a marker can support target engagement in preclinical studies, show pathway modulation in early human studies, or help rank compounds without serving as a clinical diagnostic test.
It is also useful to distinguish biomarkers from endpoints:
That distinction matters because teams often overestimate what a biologically plausible signal can support. A marker may be mechanistically relevant but still unsuitable for downstream decisions if the assay lacks fit-for-purpose performance, the analyte is unstable, or the signal changes across matrices or timepoints in ways that complicate interpretation.
Major Biomarker Categories and Their Research Roles
Biomarker categories are most useful when they are defined by the decision they are meant to inform.
Diagnostic Biomarkers
A diagnostic biomarker supports detection or classification of a disease or condition. In research, these markers may help distinguish affected from unaffected samples, refine cohort definitions, or compare molecular subtypes. Work in this category often requires close attention to analytical specificity because related disease states can produce overlapping signals.
Prognostic Biomarkers
A prognostic biomarker is associated with future disease course independently of a specific therapy. These markers are commonly studied in natural history cohorts, risk models, and disease progression analyses. Prognostic use usually depends on longitudinal evidence and careful control of confounders; a cross-sectional association alone is rarely sufficient.
Predictive Biomarkers
A predictive biomarker identifies the likelihood of differential response to a therapy. This category is central to patient stratification, enrichment strategies, and some companion diagnostic pathways. A predictive claim requires more than a link to disease biology. The evidence must support that treatment effect differs across biomarker-defined subgroups.
Pharmacodynamic Biomarkers
A pharmacodynamic biomarker reflects a biological response after treatment or exposure. These markers are often used to assess target engagement, dose selection, mechanism support, and translational bridging between preclinical and clinical studies. Timing is especially important because the relevant signal may be transient and strongly affected by the sampling window.
Safety Biomarkers
A safety biomarker indicates a biological response related to toxicity or tissue injury. In research programs, such markers may help compare compound liabilities, track off-target effects, or support nonclinical-to-clinical translation. The analytical challenge often lies in selectivity, since many injury-associated markers rise in more than one pathological context.
Exploratory and Translational Biomarkers
Exploratory biomarkers are early-stage candidates that still require technical and biological clarification. In translational research, this stage often begins with omics-derived candidate lists. At that point, teams should separate three concepts that are often blurred together:
Where Biomarkers Are Applied Across Drug Development and Medical Research
Biomarkers appear throughout biomedical R&D, but the role of the marker changes as the program moves from hypothesis generation to higher-stakes decisions.
Discovery and Mechanism Studies
In early discovery, biomarkers connect pathway biology to measurable outputs. A phosphorylation event, transcript signature, metabolite ratio, or cellular phenotype may show whether a perturbation affects the intended mechanism. At this stage, multiplex methods are often attractive because they preserve breadth while the biology is still being mapped.
Preclinical Model Evaluation
In animal models and ex vivo systems, biomarkers are used to compare mechanisms, rank leads, or characterize pharmacology. The question is not only whether the signal changes, but also whether the model and matrix support later translation. A tissue biomarker may be mechanistically strong in preclinical work but difficult to sample repeatedly in humans. A circulating marker may be more practical but less proximal to the pathway of interest.
Early Clinical Translation
In early human studies, biomarkers often support dose selection, target engagement, pathway modulation, and exposure-response analysis. Here, sample timing, analyte stability, and cross-site handling can become major sources of variability. Translational biomarkers must perform under more heterogeneous workflows than they do in tightly controlled discovery settings.
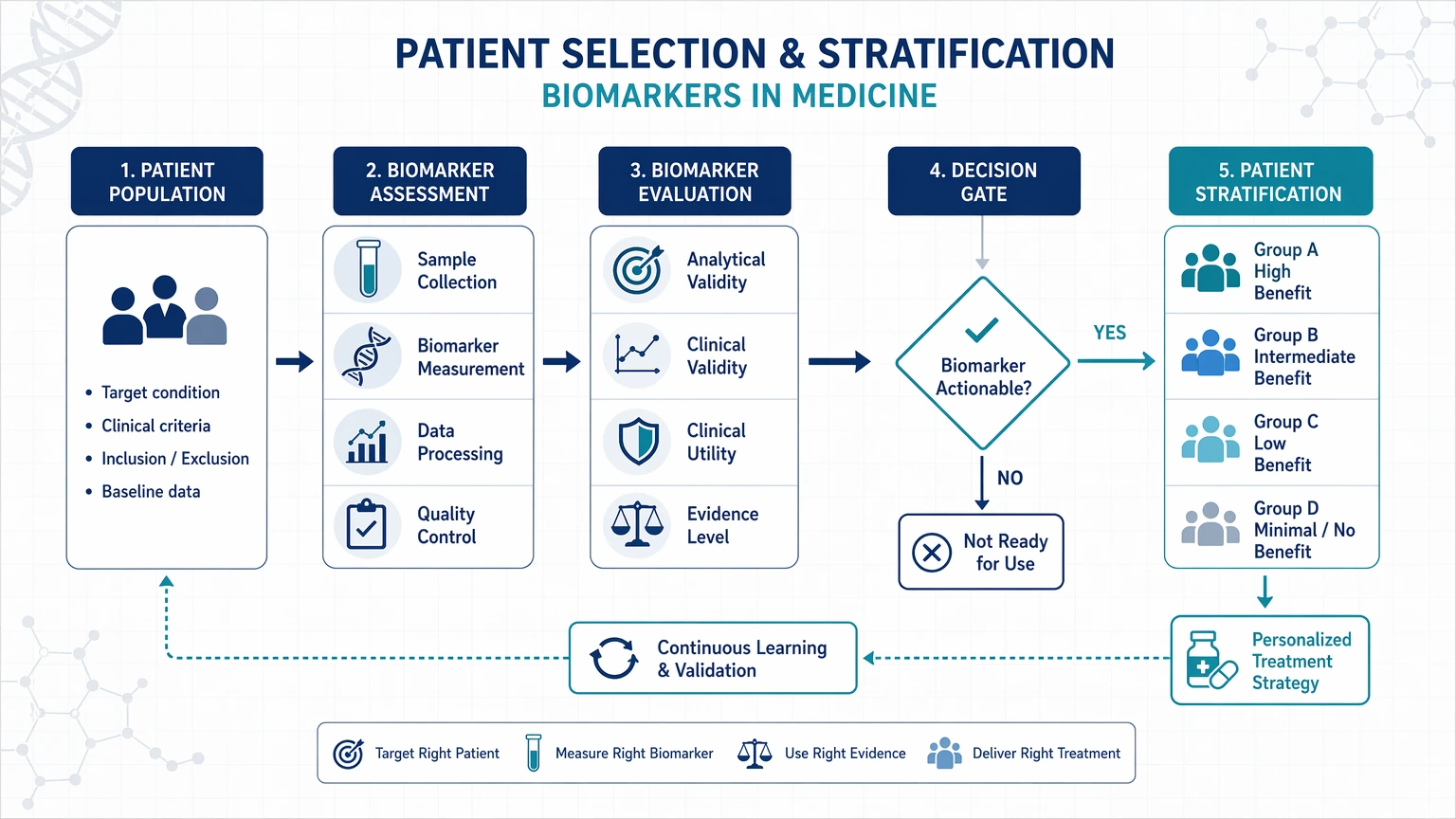
Patient Selection and Stratification
When a program uses a biomarker for enrollment, subgroup definition, or treatment allocation, the assay must be tightly linked to the intended decision. That increases the importance of specificity, cutoff strategy, and inter-run comparability. Tissue-based markers may introduce scoring variability or pathologist-dependent interpretation. For circulating genomic markers or liquid biopsy assays, low abundance and preanalytical losses may be limiting.
Monitoring and Resistance Tracking
Serial biomarker measurements can support treatment monitoring, disease progression assessment, and resistance tracking. Longitudinal use shifts attention toward repeatability, lot-to-lot consistency, normalization, and missing-data patterns. A marker that is informative in a single cross-sectional comparison may still be unsuitable for longitudinal interpretation if storage effects, baseline drift, or batch structure are not well controlled.
Service Routes for Study Planning
For teams moving from method selection into execution, these service paths connect assay design, validation, and interpretation needs.
Common Analytical Platforms for Biomarker Measurement
No analytical platform is optimal for every biomarker class. Platform selection should match molecular form, abundance, specimen matrix, throughput, and whether the study needs broad profiling or focused quantitation.
LC-MS/MS and Targeted Mass Spectrometry
Mass spectrometry is commonly used for proteins, peptides, metabolites, lipids, and modified analytes when molecular specificity is a priority. Targeted LC-MS/MS can support multiplexed quantitation with internal standards and can serve as an orthogonal method for confirming immunoassay findings. Method planning should address extraction recovery, ion suppression, matrix effect, carryover, and dilution integrity where relevant.
Immunoassays
ELISA and related immunoassays are often used when a protein biomarker has suitable affinity reagents and a concentration range compatible with the assay. These methods are efficient for focused measurement, but their limitations can include cross-reactivity, epitope dependence, heterophilic interference, and reduced ability to distinguish isoforms or closely related analytes.
Flow Cytometry
Flow cytometry is useful for cell-state biomarkers, immune phenotyping, and receptor occupancy studies. It provides single-cell resolution, but panel design, compensation, gating strategy, viability effects, and specimen handling all influence reproducibility. The assay readout depends not only on instrumentation but also on a well-controlled analysis strategy.
qPCR and ddPCR
qPCR and ddPCR are widely used for nucleic acid biomarkers, copy number analysis, rare mutation tracking, and transcript quantitation. ddPCR can be helpful at low abundance, while qPCR remains practical for many targeted applications. Both methods require careful control of extraction efficiency, inhibitors, and normalization to appropriate reference materials or housekeeping targets.
NGS-Based Approaches
NGS supports genomic, transcriptomic, and some epigenetic biomarkers, especially in discovery and broad profiling workflows. It can capture variant structure and pathway-level patterns, but assay complexity, library preparation, sequencing depth, and bioinformatics choices can all affect comparability. For downstream decisions, orthogonal confirmation is often warranted.
Histology, IHC, ISH, and Imaging-Linked Methods
Tissue biomarkers often rely on morphology-linked methods such as histology, immunohistochemistry, or in situ hybridization. These approaches preserve spatial context and can be highly informative for mechanism and stratification, but they also introduce challenges such as fixation artifacts, scoring variability, and heterogeneity across tissue regions.
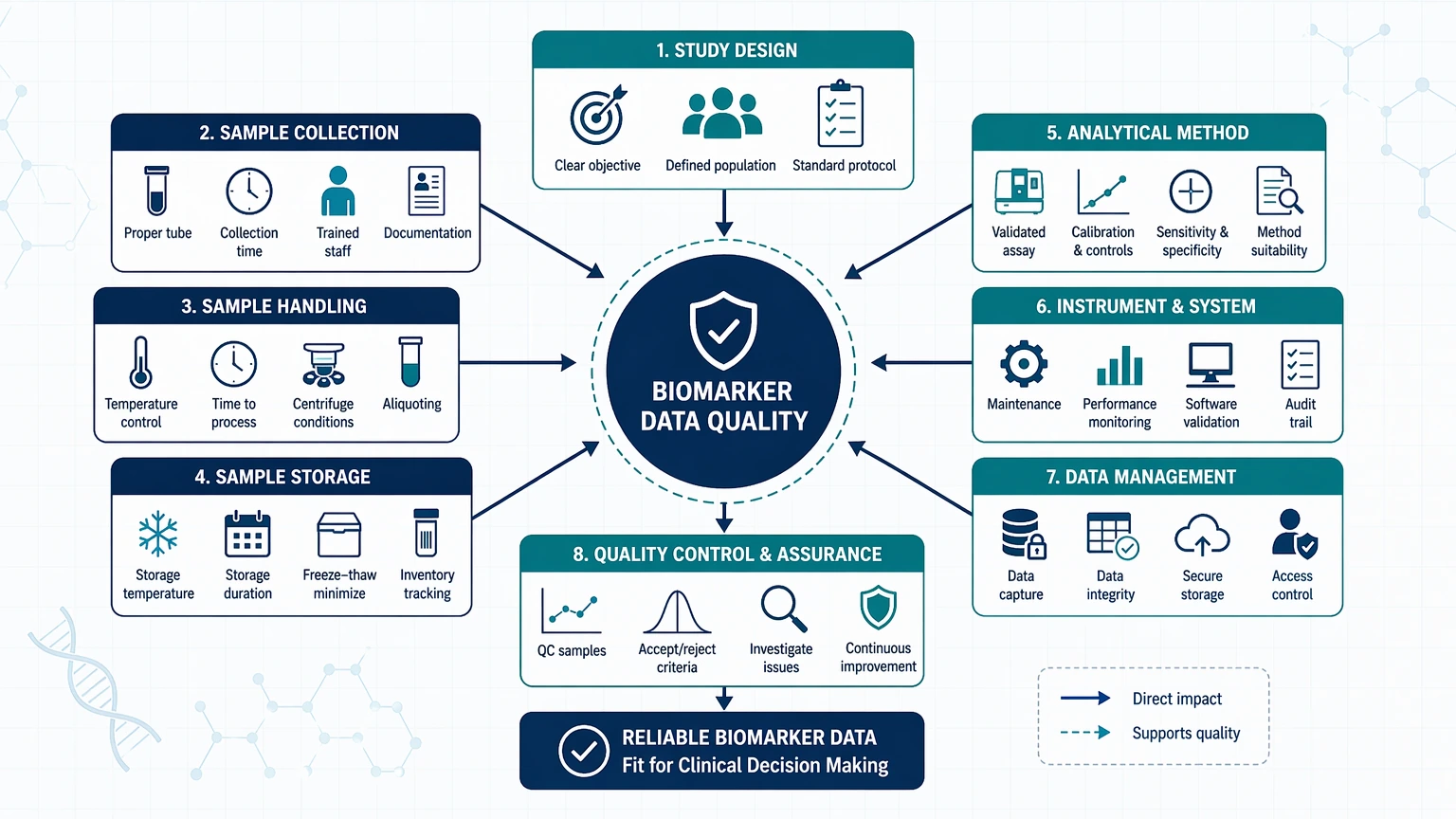
Method Considerations That Affect Biomarker Data Quality
A biologically promising biomarker can still fail if the measurement strategy is poorly matched to the sample, platform, or study objective.
Sample Matrix and Biospecimen Strategy
The selected biospecimen or specimen matrix should reflect both biology and operational feasibility. Tissue may be closest to the mechanism, plasma may support serial sampling, and urine or CSF may offer advantages in specific use cases. The key question is whether the matrix contains the analyte in a measurable and interpretable form.
Preanalytical Variability
Collection tube type, anticoagulant choice, clotting time, centrifugation delay, freeze-thaw exposure, storage duration, and shipping conditions can all change biomarker measurements. Preanalytical variability should be treated as part of study design rather than a downstream troubleshooting issue.
Sensitivity and Lower Limits
Low-abundance biomarkers require methods with adequate analytical sensitivity and clear definitions of LOD and LLOQ. Teams should ask whether expected baseline or post-dose concentrations fall within the quantifiable range and whether rare positive findings can be distinguished from background noise.
Specificity and Selectivity
A biomarker assay should separate the intended analyte from related molecules, degradation products, endogenous interferents, or matrix background. Specificity problems often arise when a method captures a family of molecules rather than the exact molecular form tied to the biological hypothesis.
Precision, Accuracy, and Reproducibility
Interpretation becomes weak when assay variability approaches the size of the biological effect. Precision should be evaluated within runs and across runs. Accuracy can be assessed when reference materials or an orthogonal method are available. Reproducibility across operators, instruments, sites, or reagent lots becomes more important as studies scale beyond a pilot phase.
Dynamic Range, Linearity, and Upper Limits
Biomarker concentrations can span wide ranges across dose levels, disease states, or patient subgroups. A method should have enough dynamic range to quantify low and high signals without excessive sample rework. Linearity and ULOQ are especially relevant when response magnitude or disease burden can drive concentrations upward.
Recovery, Stability, and Carryover
For many workflows, analytical interpretation also depends on extraction recovery, short- and long-term stability, and platform-specific carryover. If the analyte degrades during handling or if residual signal affects subsequent injections or wells, the reported value may no longer reflect the original sample state.
Normalization and Batch Control
Normalization should be defined before data lock. Acceptable strategies may include housekeeping genes, isotopically labeled internal standards, spike-ins, total protein correction, or reference materials. Batch effects should be tracked with controls and bridging samples, particularly in multi-phase studies or multi-site programs.
How to Match Biomarker Purpose to Study Design
The biomarker plan becomes clearer when study design is organized around the decision the marker is expected to support.
Tradeoffs are unavoidable. A multiplex assay may preserve information breadth in discovery, but it also increases the risk of cross-reactivity, calibration complexity, and panel interference. A single-analyte assay may provide cleaner quantitation once one marker has been prioritized. Likewise, tissue biomarkers may capture local biology better than blood-based assays, while circulating assays may be better suited for repeated sampling. The most useful design is the one that keeps measurement capability aligned with the program decision.
For teams comparing platforms or defining validation scope before study launch, a focused technical review can reduce redesign later. In that setting, you can submit your requirements to MtoZ Biolabs for a biomarker assay planning discussion tied to sample constraints, analyte class, and study stage.
Practical Questions to Ask Before Starting a Biomarker Study
Before a biomarker study begins, teams should test the plan against a short set of technical and biological questions:
These questions help separate a biologically interesting marker from one that is ready for a defined analytical workflow.
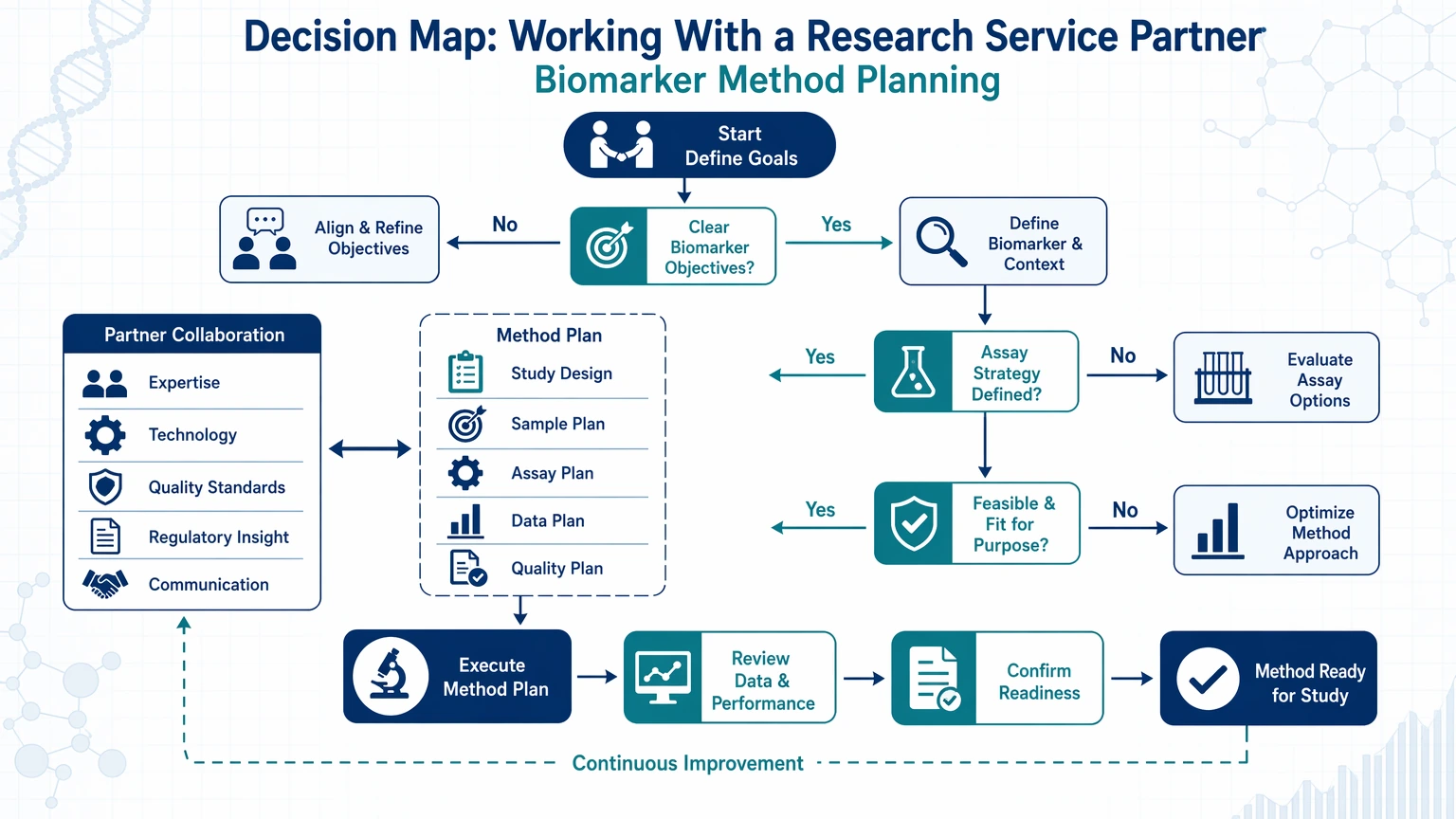
Working With a Research Service Partner on Biomarker Method Planning
External analytical support is often most useful when a team has candidate markers but still needs to connect biology, sample strategy, and assay format. A productive discussion with a research partner usually covers:
In this context, the value of a partner is not a universal platform recommendation. It is the ability to compare feasible methods against the actual study question and identify where assay readiness may limit interpretation. If your team is selecting between targeted mass spectrometry, immunoassays, molecular assays, or tissue-based workflows, contact us at MtoZ Biolabs to evaluate your project in the context of biomarker purpose, sample access, and analytical boundaries.
Conclusion
Biomarkers in medicine are most useful when biological meaning and measurement strategy are developed together. The right path begins with context of use, then links biomarker category to matrix choice, platform fit, and study design. Before acting on a biomarker result, teams should examine sensitivity, specificity, precision, reproducibility, dynamic range, matrix effect, stability, normalization, and preanalytical control in the setting where the assay will actually be used.
Some programs justify broad exploratory panels, while others are better served by targeted assays with tighter quantitative control. The central planning question is not which platform is best in general, but which method can generate interpretable data for the decision at hand.
FAQ
How is biomarker verification different from biomarker validation?
Verification asks whether a candidate biomarker can be measured reproducibly in the relevant sample type and whether the observed signal persists outside the original discovery set. Validation goes further by establishing the evidence needed for the intended use. That may involve fit-for-purpose studies, broader analytical characterization, and, in later settings, clinical validation. A marker can pass discovery yet fail verification if the assay cannot separate true biology from matrix background or handling-related variability.
When is a tissue biomarker preferable to a circulating biomarker?
A tissue biomarker is often preferred when spatial context, local pathway activation, or cell-type-specific expression is central to the question. A circulating biomarker may be more practical when repeated sampling, treatment monitoring, or lower collection burden matters more than direct tissue proximity. The tradeoff is straightforward: tissue can be closer to mechanism, while blood-based measurements are often easier to collect serially but may show dilution, background signal, or contributions from non-target tissues.
Why do promising discovery biomarkers fail during assay development?
Many candidates fail because the original signal does not translate into a stable, measurable assay. Common reasons include low abundance, poor reagent selectivity, matrix interference, degradation during handling, inconsistent normalization, or differences between discovery cohorts and follow-up samples. Discovery identifies candidates; assay development tests whether the candidate survives real analytical constraints.
Is multiplexing always the right choice in translational biomarker studies?
No. Multiplexing is useful when sample conservation, pathway breadth, or exploratory mapping is the main goal. It becomes less attractive when cross-reactivity, panel interference, calibration burden, or data interpretation complexity outweigh the benefit of measuring additional analytes. Once one biomarker is tightly linked to a program decision, a targeted assay may be easier to characterize and control.
Which performance characteristics should be checked before a biomarker informs a major study decision?
The core set usually includes sensitivity, specificity, precision, reproducibility, dynamic range, stability, and matrix effect. The priority within that set depends on the context of use. For a low-abundance circulating marker, LOD and LLOQ may dominate. For longitudinal monitoring, inter-run comparability and normalization may be more important. For tissue assays, sampling heterogeneity and scoring reproducibility can become major constraints.
How to order?

