
Deep Sequencing and Human Antibody Repertoire Analysis: How to Plan a Study for Vaccine Response or Immune Monitoring
- baseline samples are available, but post-dose timing is too sparse to follow clonal expansion or persistence
- PBMCs were collected for convenience, but later discussions shift toward enriched B cells or antigen-specific B cells
- IGH-only profiling was chosen first, but downstream teams later ask for paired heavy/light chain information for antibody reconstruction
- sequencing depth becomes the main topic before the group agrees on the actual endpoint, such as clonotype tracking, repertoire diversity, V gene and J gene usage, SHM burden, or clonal lineage analysis
- detect vaccine-associated clonal expansion between baseline and an early follow-up
- compare repertoire diversity before and after intervention
- monitor persistence or recall-like behavior across longitudinal sampling
- recover candidate sequences for later recombinant re-expression
- look for convergent clonotype patterns across subjects
- the project may move selected sequences into recombinant re-expression
- paired heavy/light chain information is needed rather than inferred
- clonal lineage interpretation depends on fuller variable region context
- the team expects sequence recovery that can support downstream confirmation
- clonotype counts and clone frequency distributions
- repertoire diversity
- repertoire overlap across timepoints
- CDR3 length distributions
- V gene and J gene usage
- SHM burden summaries
- clonal lineage clustering
- convergent sequence patterns across subjects
- What sample type will be collected at each timepoint?
- Is the study using bulk repertoire sequencing, broader variable region recovery, or a workflow aimed at paired heavy/light chain information?
- Which outputs are required for the report, and which are exploratory only?
- What validation, if any, is expected after sequence recovery?
- How will batch handling, metadata completeness, and replicate strategy be controlled across visits?
A human antibody repertoire study should begin with the decision it needs to support, not with a sequencing menu. For vaccine response or immune monitoring, the strongest studies usually use longitudinal sampling with a baseline and more than one post-intervention timepoint. One snapshot alone cannot show clonal expansion, repertoire overlap over time, or changes in somatic hypermutation (SHM).
If the goal is cohort-level immune monitoring, bulk repertoire sequencing from PBMCs may be enough. If the project needs cleaner B-cell receptor repertoire resolution, stronger sequence recovery for follow-up, or a realistic path to recombinant re-expression, the study should define B-cell enrichment or antigen-specific B cells early. It should also decide whether immunoglobulin heavy chain (IGH) alone is enough or whether paired heavy/light chain information from IGH plus immunoglobulin kappa chain (IGK) or immunoglobulin lambda chain (IGL) is required.
Where Study Planning Usually Breaks Down
Most planning problems show up before sequencing starts. Teams often lock collection windows, freezer inventory, and budgets before they agree on what the dataset needs to answer. Once that happens, the workflow starts driving the question instead of supporting it.
In vaccine response or immune monitoring studies, the same four issues come up again and again:
These mismatches do more than narrow interpretation. They also shape whether the dataset can support the next project decision, such as adding follow-up validation, changing the cohort schedule, or selecting clones for further work.
The Four Design Decisions That Matter Most
1. Define the endpoint before you choose the workflow
The first design question is straightforward: what does this study need to decide?
That answer should be narrow and reportable. For example:
Each objective pushes the design in a different direction. Bulk repertoire sequencing can often support clonotype frequency tracking, repertoire overlap, and diversity trends. A study that may move selected sequences into binding work or recombinant re-expression usually needs broader variable region recovery and earlier attention to pairing limits.
2. Match the sampled compartment to the biological question
Sample source determines which part of the human antibody repertoire you can interpret with confidence.
| Sample source | Best fit | Main strength | Main limitation |
|---|---|---|---|
| PBMCs | Longitudinal cohort studies | Practical serial collection | B-cell signal is diluted by other cells |
| Enriched B cells | BCR repertoire-focused analysis | Stronger B-cell representation | Extra processing and input demands |
| Sorted antigen-specific B cells | Targeted follow-up on known antigens | Closer link to the antigen question | Requires sorting strategy and tighter sample control |
| Archived mixed blood compartments | Retrospective feasibility work | Uses available material | Cross-sample comparability may be limited |
PBMCs are often the right choice when the goal is relative change over time at the cohort level. They are less convincing when low-frequency clonotypes matter, cryopreservation quality varies, or the team wants cleaner B-cell-focused interpretation. Enriched B cells make more sense when the study is centered on the B-cell receptor repertoire itself rather than on general blood-based feasibility.
3. Decide how much chain resolution you actually need
Not every vaccine response study needs full pairing. If the main output is clonotype abundance shifts, complementarity-determining region 3 (CDR3) distributions, repertoire diversity, or V(D)J recombination patterns, IGH-only profiling can be a sensible choice.
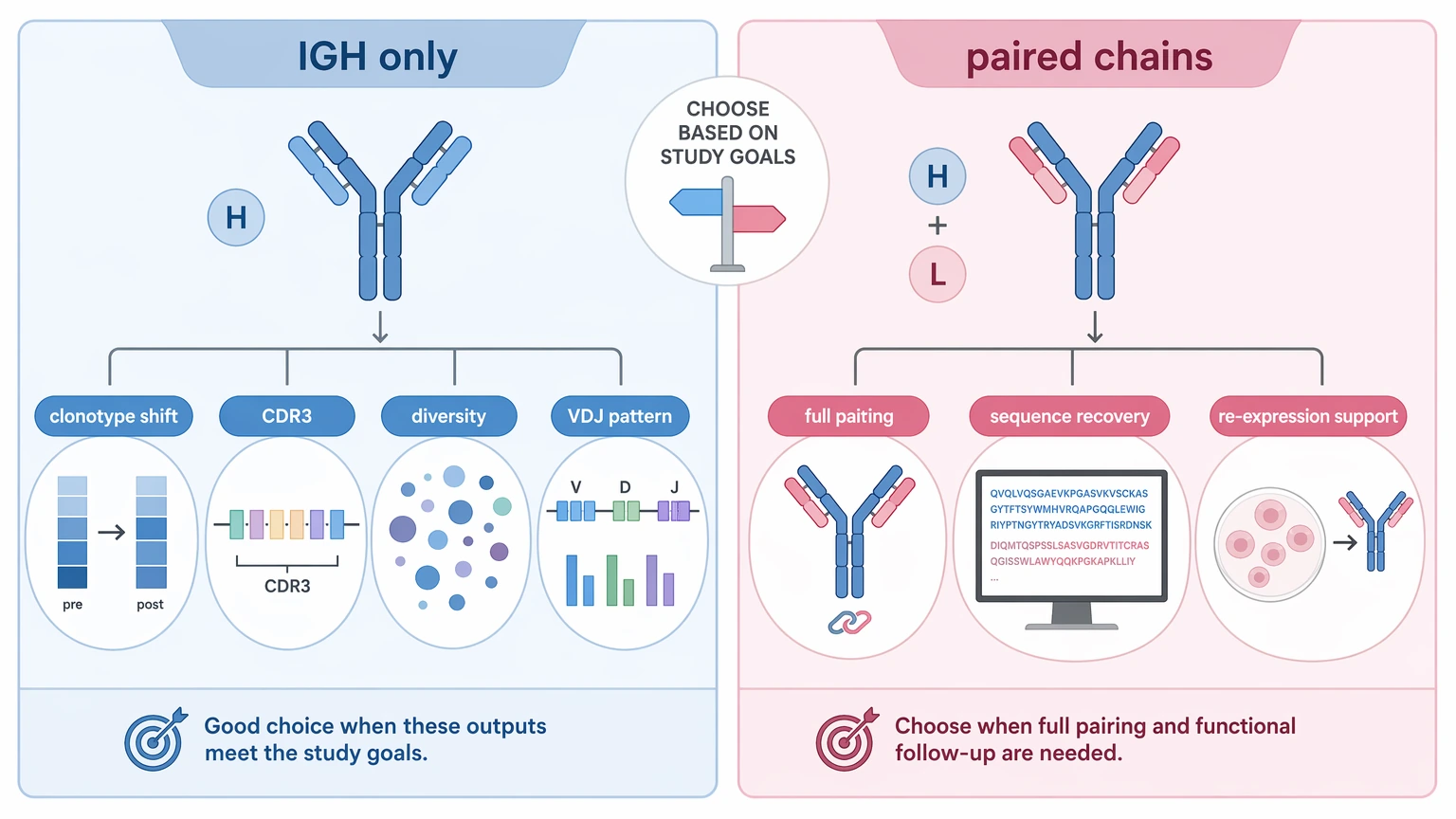
You should consider a broader design when one or more of the following are true:
This is also where CDR3-focused profiling and broader variable region recovery start to separate. CDR3-centered datasets work well for clonotype tracking. Broader recovery becomes more useful when lineage branching, SHM context, or follow-up expression work is already part of the study plan.
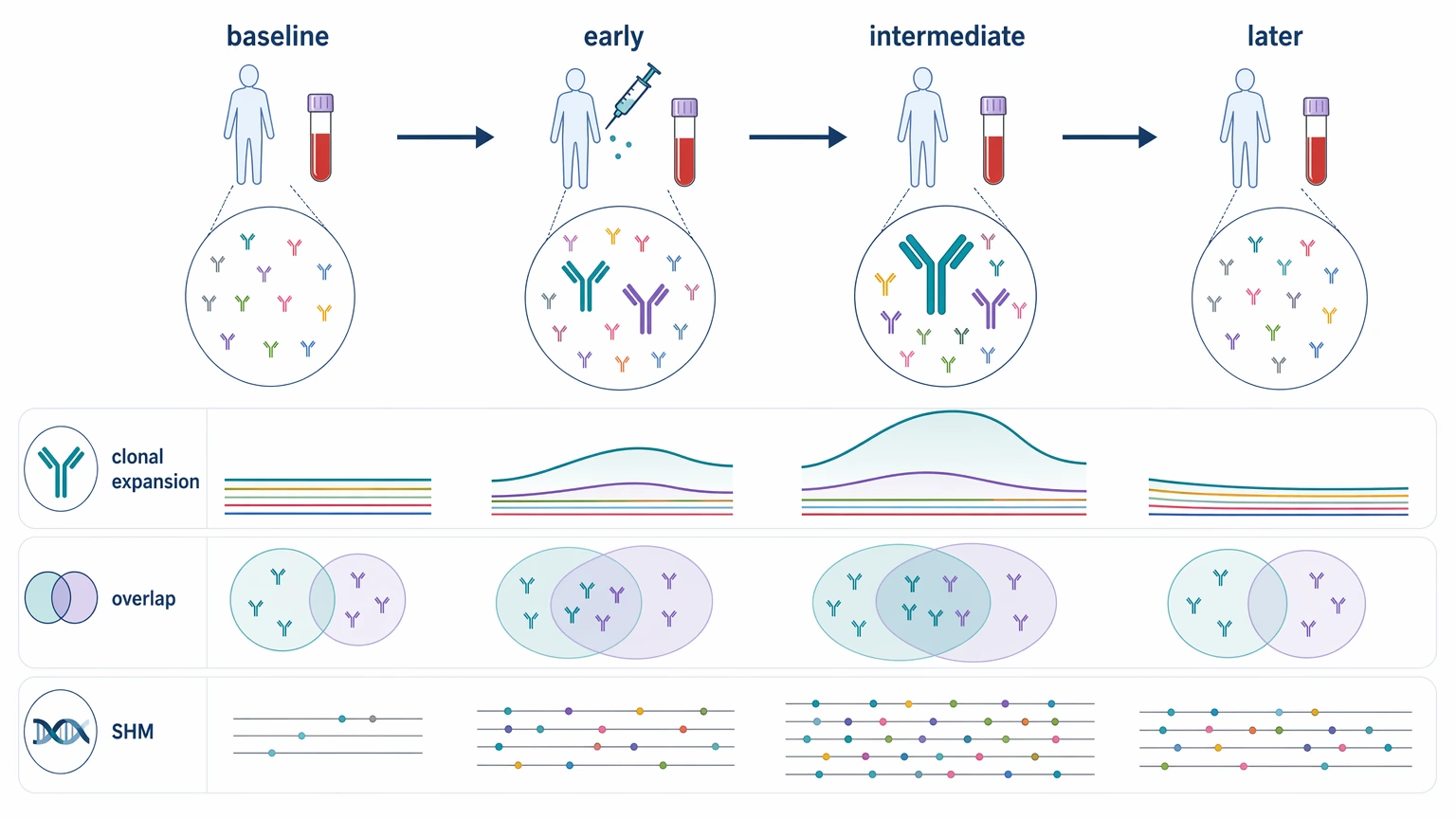
4. Build longitudinal sampling around the immune event
Longitudinal sampling is not a minor add-on. It determines which biological changes the study can actually capture.
| Timepoint role | Why include it | What it can support |
|---|---|---|
| Baseline | Defines the pre-intervention repertoire | Pre/post comparison and repertoire overlap |
| Early post-intervention | Captures emerging clonal expansion | Early clone frequency shifts |
| Intermediate follow-up | Adds maturation context | SHM summaries and clonal lineage change |
| Later follow-up | Tests persistence or contraction | Durable overlap and population turnover |
A single post-vaccination sample can describe a repertoire state at one moment. It cannot show whether a clonotype expanded quickly, persisted, contracted, or reappeared after recall. For that reason, more than one post-intervention draw is usually more informative than one late sample when the study question is about dynamics.
At this stage, it can help to submit your requirements and evaluate your project with MtoZ Biolabs if the team is still weighing PBMC input, B-cell enrichment, timepoint density, or sequence-recovery scope.
How to Turn Those Decisions Into a Practical Study Plan
Step 1: Write the reporting endpoint first
Before anyone starts discussing platforms, write one sentence that defines the final output. For example: “We need to compare baseline and post-dose clonotype expansion in PBMC-derived repertoires,” or “We need candidate sequence recovery that can feed recombinant re-expression.” That sentence becomes the filter for every later choice.
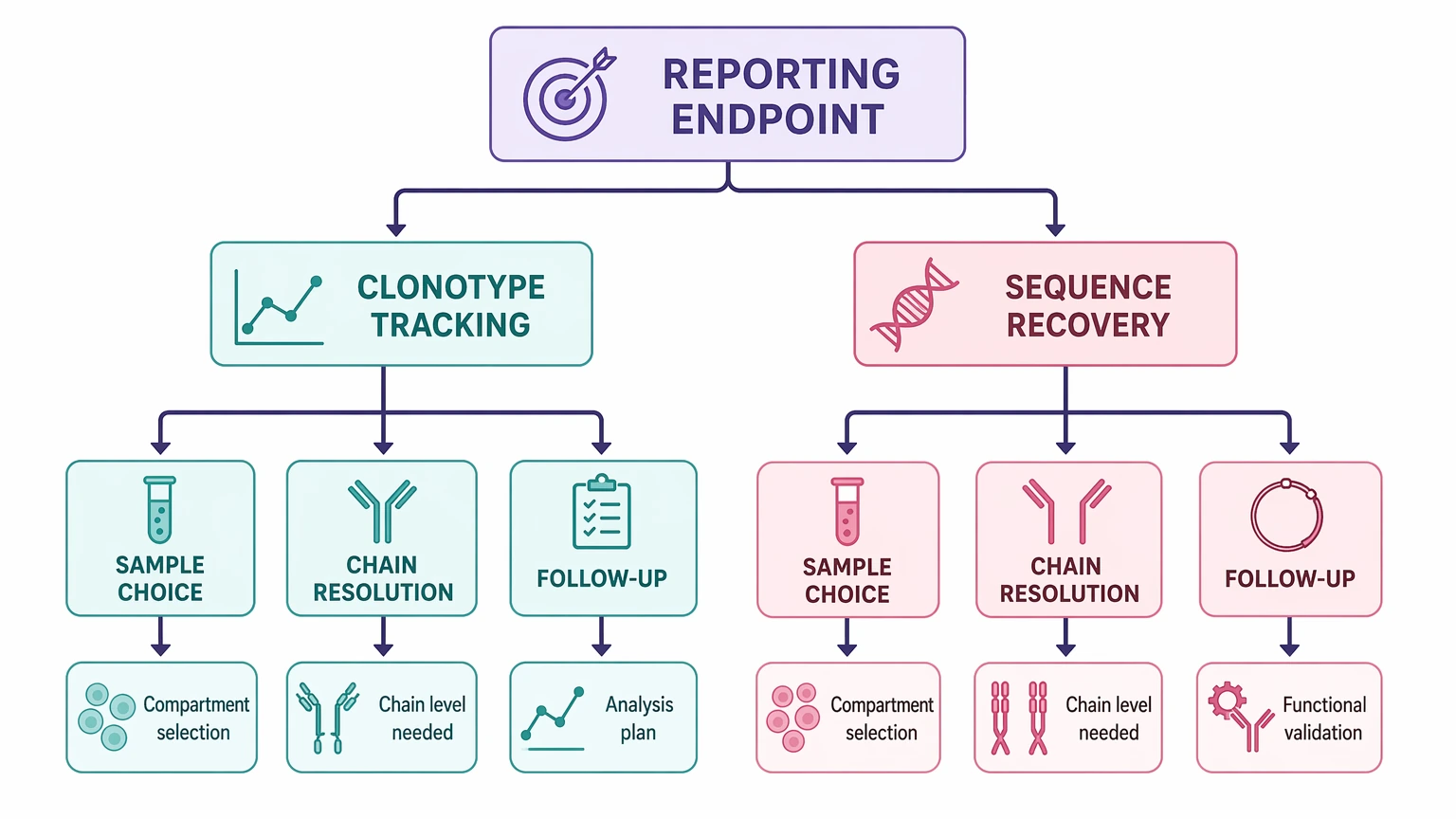
Step 2: Choose the smallest defensible biological compartment
Use PBMCs when the study is about longitudinal immune monitoring at scale. Move toward enriched B cells or antigen-specific B cells only when the planned interpretation really needs that narrower compartment. Convenience should not decide the input, but neither should an overly ambitious sorting plan that the sample reality cannot support.
Step 3: Set the analytical readout before discussing sequencing depth
Depth only means something once the readout is fixed. Common repertoire outputs include:
These outputs do not all follow the same design logic. A study focused on repertoire diversity and high-frequency clonal expansion is asking a different technical question from a study meant to deliver candidate antibodies for downstream testing.
Step 4: Add error control where low-frequency interpretation matters
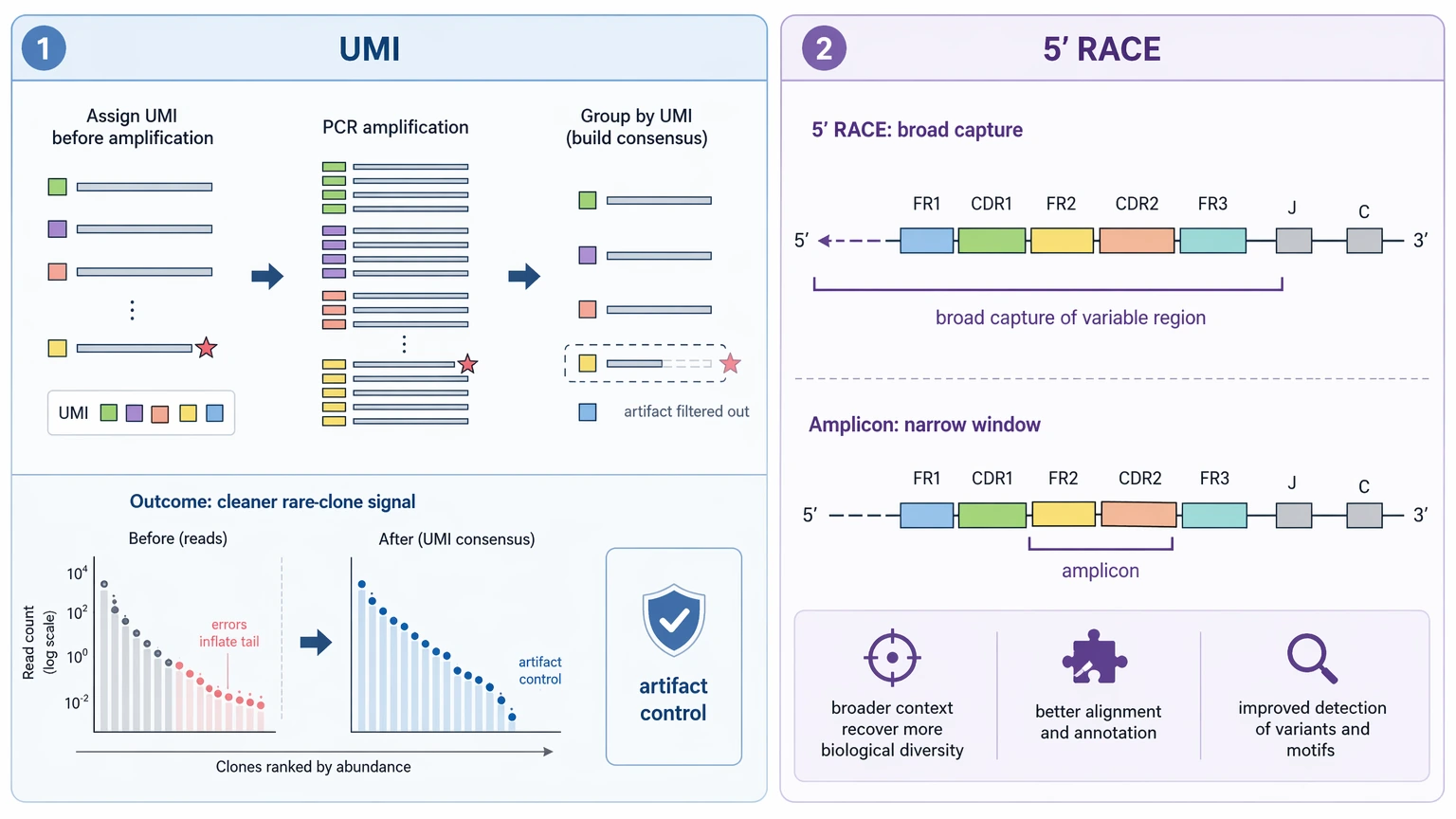
If the analysis depends on rare clonotypes or subtle changes across timepoints, error-aware designs matter. A unique molecular identifier (UMI) can improve confidence that low-frequency observations are not dominated by amplification or sequencing artifacts. Likewise, 5' RACE can be useful when broader variable region capture matters more than a narrowly defined amplicon target.
Step 5: Set interpretation boundaries before the report is written
This step prevents the most common overreach. Bulk repertoire sequencing can show that clonotypes expand, persist, overlap across visits, or accumulate SHM-associated variation. It does not, by itself, prove antigen specificity, neutralization, protection, or clinical benefit.
| Repertoire observation | Reasonable interpretation | What still needs follow-up |
|---|---|---|
| Clonal expansion after intervention | Consistent with vaccine-associated B-cell activity | Antigen specificity and functional relevance |
| Greater repertoire overlap across visits | Consistent with persistence of detectable clonotypes | Biological importance of those clones |
| Higher SHM burden in selected lineages | Consistent with ongoing maturation | Binding and functional consequences |
| Convergent clonotype-like patterns across subjects | Suggests shared repertoire features | Direct antigen-linked confirmation |
If downstream stakeholders are likely to ask for clone-specific evidence, plan that path early. Orthogonal binding assays, targeted cell sorting, monoclonal characterization, and selective recombinant re-expression all start from different assumptions than bulk repertoire reporting alone.
What a Study-Ready Plan Should Include
Before samples are committed, the team should be able to answer these questions clearly:
A plan that answers those points usually leads to a dataset that is easier to interpret and easier to defend in later program discussions.
Key Constraints to Keep in View
Sample integrity still sets practical limits. Nucleated-cell quality, RNA quality for RNA-based workflows, cryopreservation consistency, and nucleic acid input all affect whether enrichment, sorting, or broader recovery is realistic.
Batch effects matter too. Even a strong longitudinal design becomes harder to interpret if baseline and follow-up samples move through different handling conditions without tracking. In immune monitoring studies, metadata discipline is part of the analytical design, not just an administrative task.
Finally, some questions are better served by a different primary method. If the real goal is direct clone recovery, sequence confirmation from purified antibodies, or functional ranking of discrete candidates, a repertoire-level study may not be the first or best choice.
Conclusion
Deep sequencing and human antibody repertoire analysis is most useful when the study question, sampled compartment, longitudinal sampling design, chain-resolution plan, and analytical outputs are aligned before sequencing starts. For translational vaccine studies, serial immune monitoring cohorts, and exploratory clone-tracking projects, the strongest plan states clearly what repertoire data can show, what it cannot show on its own, and where orthogonal validation will still be needed. If you are preparing a study in that setting, contact MtoZ Biolabs to discuss your sample type, timepoint structure, desired readout, and follow-up goals so the workflow can be evaluated before samples are committed.
FAQ
Do I need the same sample type at every visit in a longitudinal study?
Ideally, yes. Mixing PBMCs at one visit with enriched B cells at another changes the biological compartment and can weaken direct comparison. If the study must use mixed inputs, define that limitation before analysis and keep interpretation conservative.
Is baseline always required for vaccine response studies?
Baseline is strongly preferred when the goal is to assess change after intervention. Without it, you can describe the observed repertoire at a post-dose timepoint, but you cannot directly measure subject-level expansion, contraction, or repertoire overlap from the pre-intervention state.
When is 5' RACE more useful than a standard amplicon design?
5' RACE becomes more attractive when broader variable region recovery matters more than a tightly constrained targeted panel, especially if lineage analysis or follow-up sequence work needs wider sequence context.
Can repertoire overlap between timepoints be compared across all subjects the same way?
Only if sampling, processing, and clonotype-calling rules are consistent. Cross-subject overlap summaries become harder to interpret when input compartments, handling conditions, or analytical definitions change across the cohort.
Should a vaccine-monitoring study bank extra material for follow-up work?
Usually yes, if the program may later request orthogonal validation, antigen-specific B-cell sorting, or recombinant re-expression. Reserved material can prevent a second collection effort when the first report identifies lineages worth pursuing.
What metadata are most important to preserve for later analysis?
At minimum, retain subject ID, visit timing, intervention timing, sample type, processing dates, cryopreservation history, nucleic acid workflow details, and batch identifiers. Missing metadata can limit longitudinal interpretation even when sequencing quality is acceptable.
How to order?

