
Personalized Medicine Antibody Analysis vs ELISA: Method Selection and Research Use Cases
- a defined assay format with one primary endpoint, or
- a customized analytical workflow designed to answer several linked questions
- targeted biomarker follow-up after candidate narrowing
- screening large sample sets for one predefined analyte
- comparing treatment groups or time points under a common protocol
- generating a semi-quantitative or quantitative readout for established markers
- supporting routine assay transfer within a research program
- custom immunoassay design for a specific sample matrix
- comparative testing across patient subgroups
- specificity and cross-reactivity assessment
- affinity or binding characterization
- confirmation of ELISA findings with an orthogonal method
- evaluation of matrix effect in plasma, serum, or other patient-derived materials
- multiplex or multi-attribute readouts when one endpoint is not enough
- fit-for-purpose validation for a translational use case
- use ELISA when the question is narrow
- add an orthogonal method when ambiguity appears
- move to a customized antibody analysis workflow when subgroup interpretation, specificity, or matrix behavior becomes central
Quick Answer
Choose ELISA when your study needs a focused quantitative readout for a defined analyte in a reasonably controlled sample matrix, especially for early screening, biomarker follow-up, or batch comparison. Choose a broader personalized medicine antibody analysis strategy when the key question is not only how much signal is present, but whether that signal reflects true specificity, target engagement, subgroup biology, interference, or binding differences across patient-derived samples. In many translational programs, the most practical option is a hybrid workflow: ELISA for scalable screening, followed by an orthogonal method or customized antibody analysis for ambiguous or higher-risk decisions.
What Readers Usually Mean by This Comparison
This comparison is often framed too narrowly. ELISA is a defined immunoassay format. Personalized medicine antibody analysis is not a single instrument, kit, or standardized platform. It is a broader research strategy that may combine targeted immunoassays, affinity or binding characterization, cross-reactivity review, matrix-focused testing, and tailored assay development around a translational question.
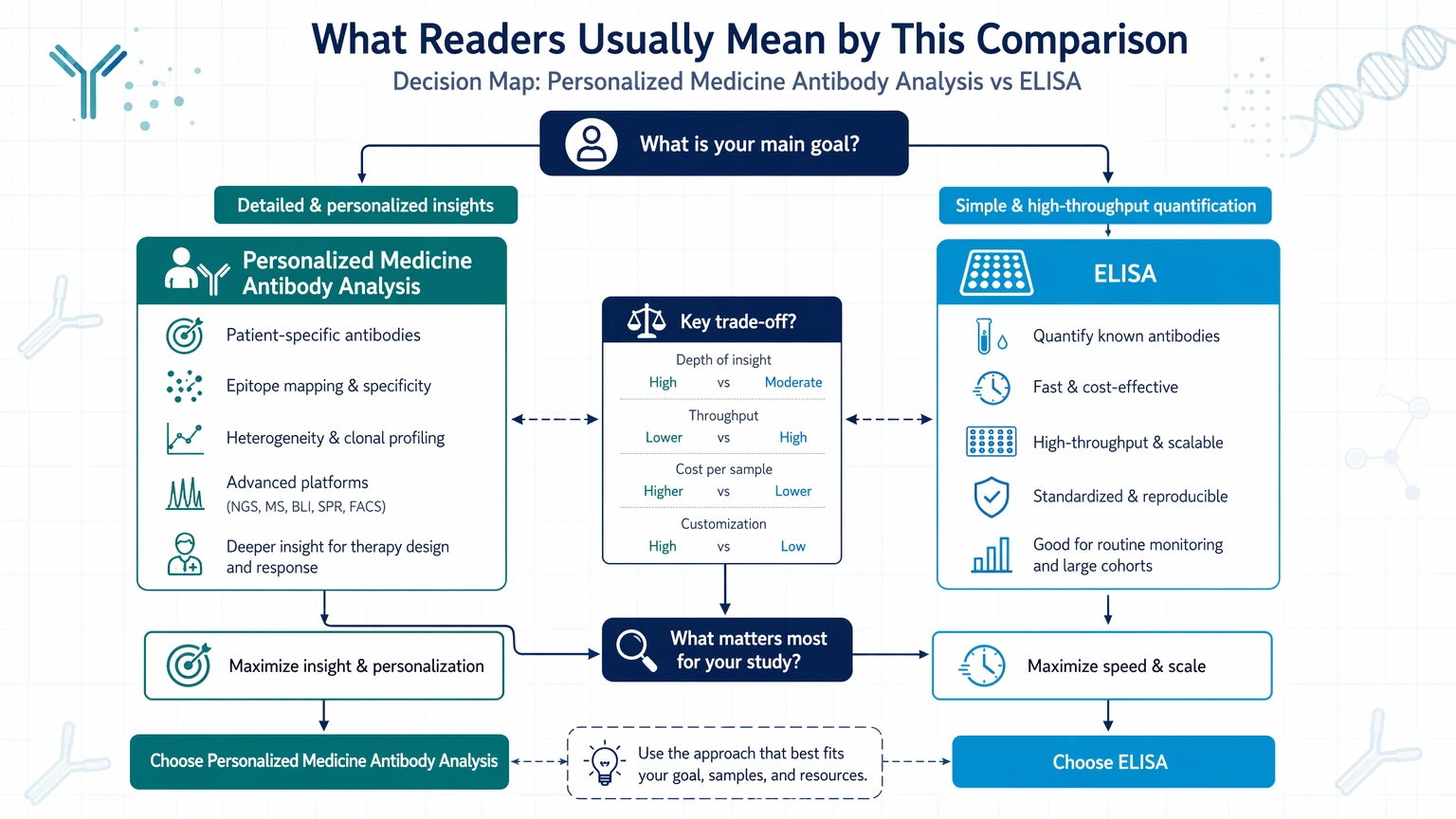
That distinction matters because most teams are not choosing between two equivalent technologies. They are choosing between:
For translational research teams working on patient stratification, biomarker-associated antibody programs, or target engagement studies, that difference affects study design, data interpretation, and downstream risk.
Where ELISA Fits in Translational Research
ELISA remains a practical choice when the biological question is narrow and the assay context is stable enough to support a targeted format. It is often a good fit when teams already know the antigen-antibody pair, the expected concentration range, and the matrix characteristics they need to control.
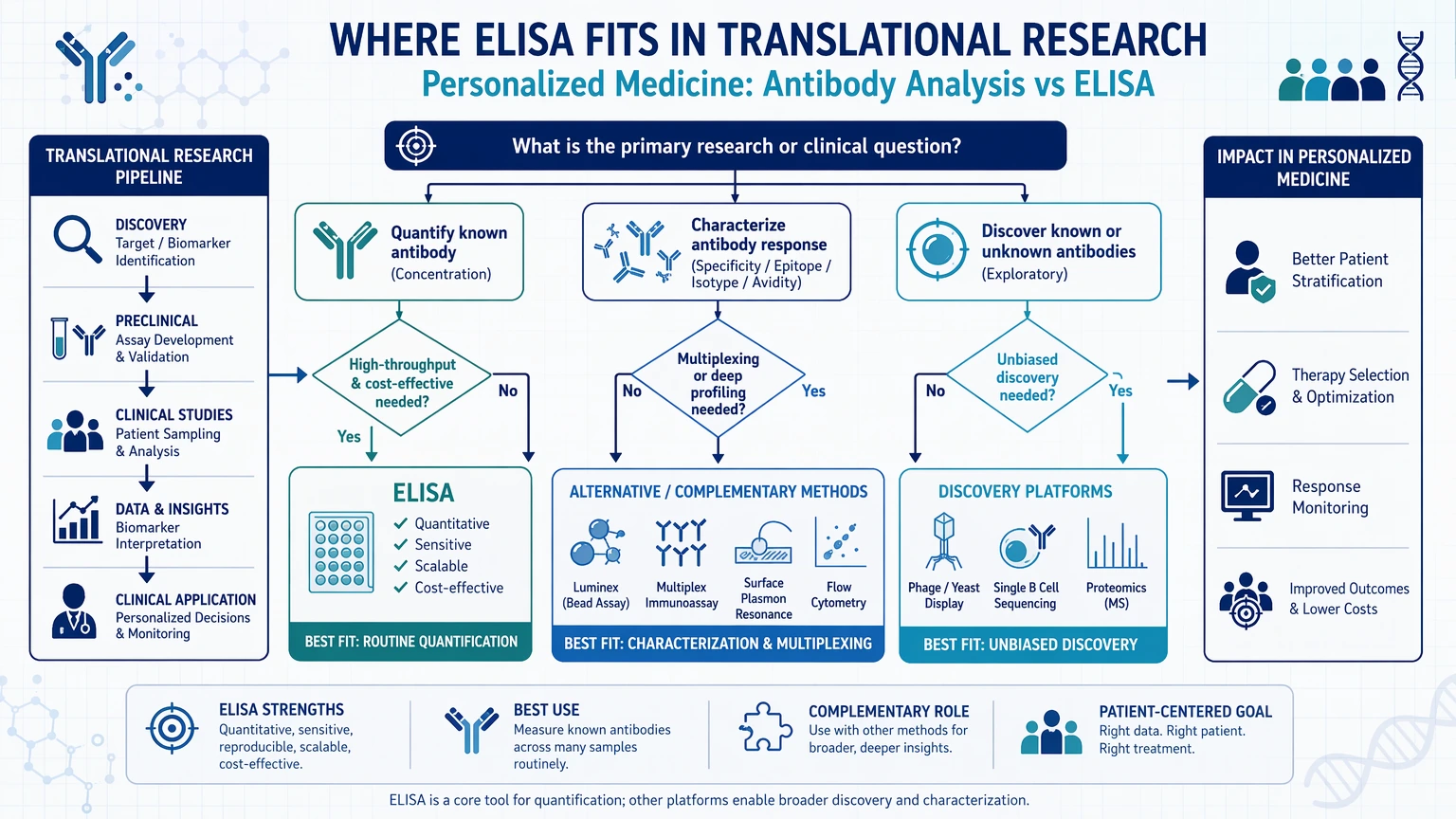
ELISA is often well suited to:
In these settings, ELISA offers clear operational advantages. It supports plate-based throughput, relatively straightforward batching, and standardized workflows when assay conditions are already understood. If the study objective is to quantify a known signal rather than explain why that signal appears, ELISA may be sufficient.
Its main limitation is scope, not usefulness. A standard ELISA result may show signal differences without clarifying whether those differences arise from true binding, epitope accessibility, off-target interaction, sample interference, or subgroup-specific biology.
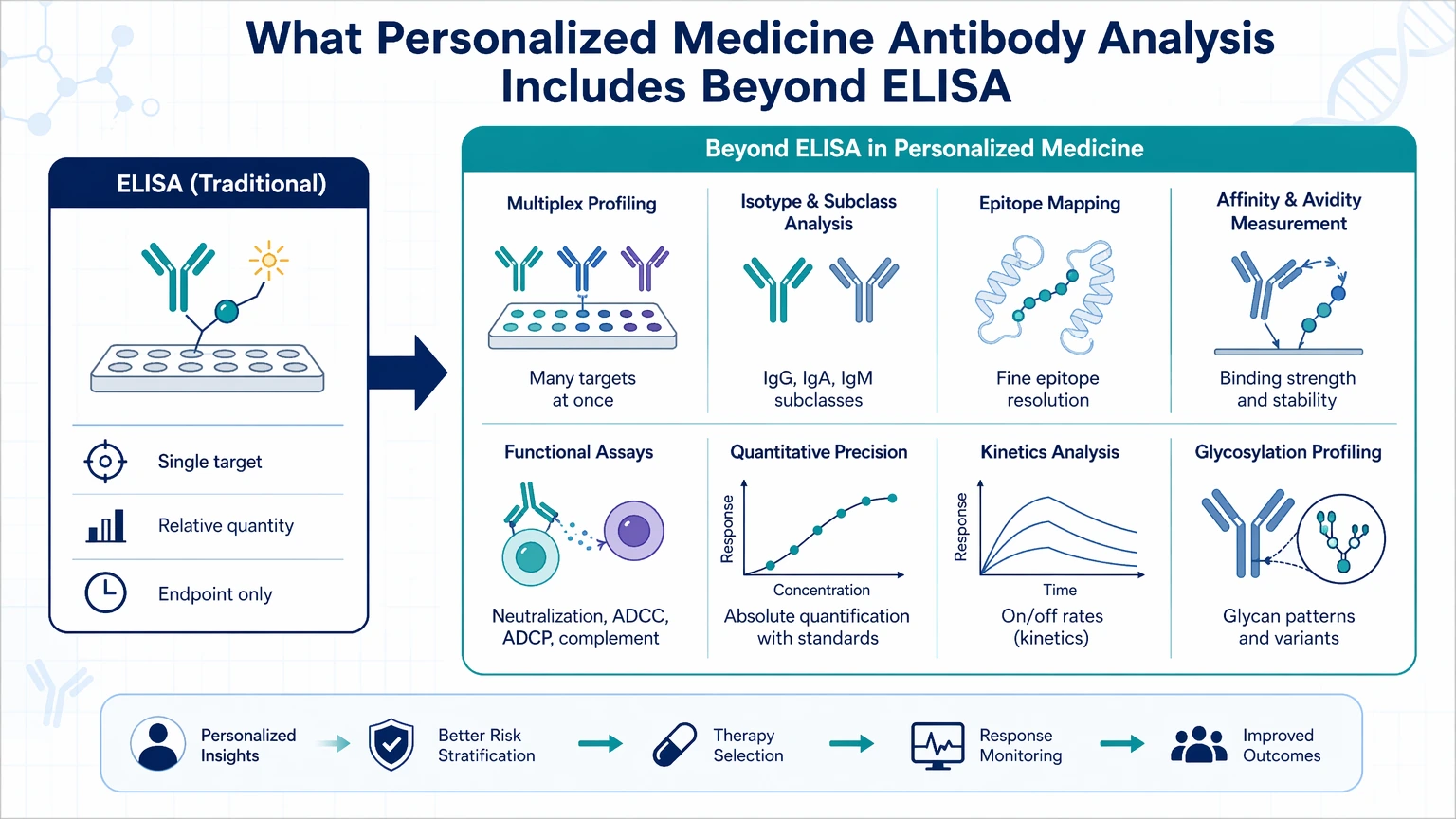
What Personalized Medicine Antibody Analysis Includes Beyond ELISA
A personalized medicine antibody analysis workflow starts with the study question and then selects methods that fit that question. In a research-service context, this may include one or more of the following:
This approach becomes more useful when the program needs interpretation rather than signal alone. For example, if one patient subgroup consistently shows a higher ELISA response, the team may need to determine whether that pattern reflects real target engagement, altered background proteins, anti-drug interference, or biological context that changes epitope exposure.
In that situation, the more useful question is not simply “Is the signal different?” but “What does this signal mean in this cohort and matrix?”
Side-by-Side Comparison
The table below summarizes the main planning implications for the method choice.
| Dimension | ELISA | Personalized Medicine Antibody Analysis |
|---|---|---|
| Basic format | Defined immunoassay | Broader analytical strategy that may combine multiple methods |
| Main output | Usually a targeted quantitative readout or semi-quantitative signal | Multi-layer interpretation that may include binding, specificity, interference, subgroup behavior, and confirmation |
| Assay flexibility | More fixed once the format is established | Greater flexibility in workflow design and readout selection |
| Throughput | Often favorable for larger sample sets | Varies by workflow and may trade throughput for data depth |
| Sample matrix handling | Can perform well in defined matrices, but matrix effect may be substantial in complex samples | Better suited when matrix-specific testing and adaptation are required |
| Specificity review | Limited unless additional controls are built in | Can explicitly include specificity and cross-reactivity studies |
| Multiplexing | Usually limited in classic ELISA formats | More adaptable when multiplexing or multi-attribute analysis is needed |
| Patient stratification support | Useful for screening known markers | Better suited to comparing biological interpretation across subgroups |
| Development burden | Lower for established assays | Higher when customization and orthogonal confirmation are needed |
| Decision risk control | Appropriate for narrow questions | Stronger when misinterpretation would affect downstream program choices |
Use these differences to align the analytical method with the biological question and validation plan.
The practical takeaway is simple: ELISA answers “how much” efficiently when the analyte and matrix are already defined well enough. Personalized medicine antibody analysis is more informative when the harder question is “what does this result mean in a heterogeneous biological context?”
Use Cases Where ELISA Is Often Sufficient
ELISA is often the right first choice when the study objective is narrow, the expected biology is already framed, and the matrix is manageable.
Defined biomarker validation steps
If a team has already selected a candidate biomarker and needs comparative quantification across samples, ELISA may provide the appropriate level of readout. This is common in follow-up studies where discovery is complete and the next question is more operational than mechanistic.
Early screening in larger sample sets
For early candidate ranking or initial screening across many patient samples, ELISA can support efficient batch processing. It is especially useful when the goal is to identify which samples or antibody candidates should advance to deeper review.
Programs with known binding pairs and limited interpretive risk
When the antibody-antigen relationship is already characterized and the cost of a mechanistic misread is relatively low, a focused ELISA may be adequate. Not every study needs epitope-level or affinity-level detail.
Stable matrix conditions
If serum, plasma, buffer, or another matrix has already shown acceptable behavior in the assay context, ELISA becomes easier to justify as a primary method.
Use Cases Where Broader Antibody Analysis Is More Informative
A customized personalized medicine workflow becomes more valuable once ELISA signals stop being self-explanatory.
Ambiguous signals in patient-derived samples
Patient materials introduce variability that can complicate interpretation. A strong signal in one subgroup may reflect true biology, but it may also reflect a matrix effect, interfering antibodies, or a different background protein profile. When that distinction matters, broader antibody analysis is usually more informative than running additional ELISA plates under nearly identical conditions.
Target engagement questions
ELISA can show signal changes associated with a target, but it may not fully resolve whether those differences reflect direct target engagement or assay behavior. If a program decision depends on that distinction, adding orthogonal antibody characterization is often justified.
Specificity and cross-reactivity concerns
When an antibody is advancing within a translational program, apparent binding alone is rarely enough. Teams may need to review specificity, examine cross-reactivity, and determine whether related proteins or matrix components influence the result.
Patient stratification and subgroup comparison
Subgroup-driven studies rarely rely on a single endpoint alone. If a biomarker program aims to compare response patterns across patient populations, the assay strategy may need to capture more than concentration. It may also need to account for binding behavior, context, and comparative interpretation across cohorts.
Multi-attribute decision points
If the project requires a combination of quantitative signal, matrix tolerance, specificity review, and possible multiplexing, a customized plan often fits better than forcing all decisions through one ELISA format.
When a Hybrid Workflow Makes More Sense Than Either Option Alone
For many teams, the practical answer is not ELISA or customized analysis by itself. It is using them in the right sequence.
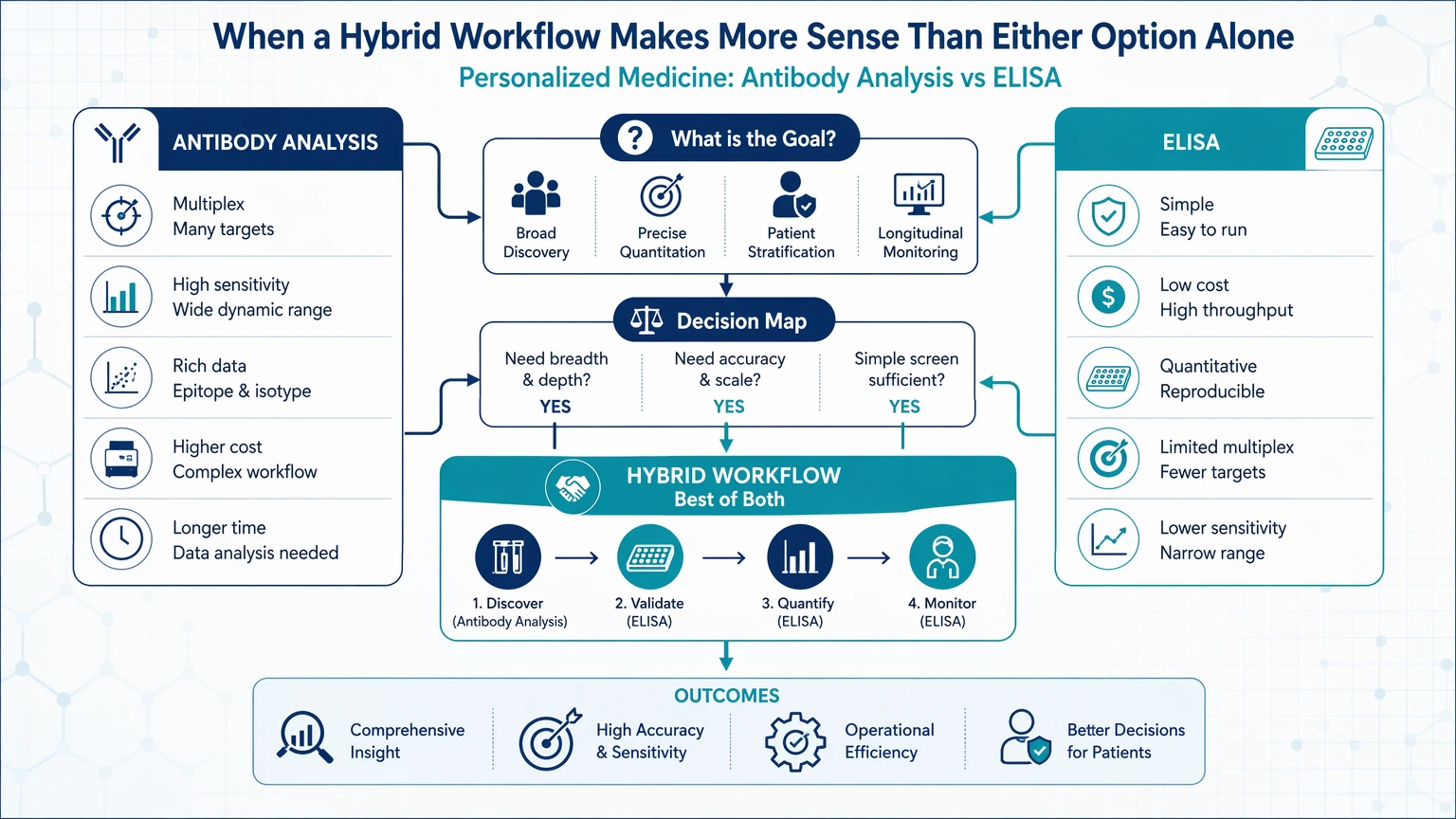
A hybrid workflow often makes sense when:
1. ELISA is used to screen large sample sets or rank candidates. 2. Outliers, subgroup differences, or discordant samples are flagged. 3. An orthogonal method is applied to clarify binding behavior, specificity, or interference. 4. The final assay strategy is narrowed for the next translational phase.
This structure helps control effort while reducing interpretive risk. It avoids under-scoping the biology and overbuilding the first assay.
A translational immunology team, for example, may begin with ELISA to compare plasma-derived samples in a patient stratification study. If one subgroup shows a distinct signal pattern, the next step may be targeted antibody analysis focused on cross-reactivity, matrix interference, or binding characterization rather than repeating the same ELISA with minor condition changes.
At that decision point, a structured project review can save time and sample. If your team needs to decide whether ELISA alone is defensible or whether a hybrid workflow is more appropriate, you can submit your requirements to MtoZ Biolabs to evaluate your project around sample matrix, subgroup structure, and reporting needs before locking in a full assay path.
Practical Selection Framework
A useful way to choose between ELISA and a broader workflow is to map the method to four operational questions.
1. What is the primary analytical objective?
Choose ELISA when the objective is targeted quantification of a known analyte.
Choose broader antibody analysis when the objective includes mechanism-level interpretation, affinity or binding characterization, or confirmation that the signal reflects the biology you think it reflects.
2. How complex is the sample matrix?
If the matrix is well behaved and prior controls suggest acceptable interference levels, ELISA may remain practical.
If the matrix is heterogeneous, patient-derived, limited in volume, or likely to contain endogenous interferents, matrix-focused assessment should be built into the workflow from the start.
3. How much interpretive risk can the program tolerate?
If a mistaken signal interpretation would mainly affect low-risk screening, ELISA may be enough.
If the result will shape candidate selection, subgroup prioritization, or later-stage translational decisions, orthogonal confirmation becomes more attractive.
4. What type of output will the team need next?
If the next step only requires rank ordering or concentration comparison, a focused assay may be sufficient.
If the next step requires evidence for specificity, understanding of cross-reactivity, or support for fit-for-purpose validation, broader analysis is usually easier to defend.
Technical Considerations to Scope Early
Method selection becomes easier when teams define several technical parameters before platform discussions expand.
Dynamic range and lower signal expectations
Any discussion of sensitivity or lower-limit performance should remain assay-dependent. The more practical planning question is whether the expected analyte range and biological spread fit the planned format without creating floor or ceiling effects.
Precision and batch comparability
For ELISA, teams should consider operator consistency, plate effects, calibrator strategy, and how reproducibility will be monitored across runs. For broader workflows, precision planning may also involve method-to-method comparability rather than plate-to-plate consistency alone.
Sample volume
When sample volume is constrained, especially in subgroup studies, the workflow should reserve material for confirmation. A one-pass ELISA plan can become limiting if ambiguity appears after screening.
Validation scope
In research-use settings, fit-for-purpose validation should match the decision being supported. A screening assay and a subgroup-interpretation assay do not need identical validation logic, but both should be scoped deliberately.
How to Avoid Under-Scoping or Overbuilding the Assay Plan
Under-scoping usually happens when a team continues using ELISA after the project has shifted from quantification to interpretation.
Overbuilding happens when a team launches a complex custom workflow before confirming that a simpler quantitative readout can answer the first program question.
A more disciplined sequence is to match analytical depth to program stage:
That staged approach is often easier to justify internally because each method addresses a defined decision point instead of trying to answer every question at once.
Service Routes for Study Planning
For teams moving from method selection into execution, these service paths connect assay design, validation, and interpretation needs.
Conclusion
ELISA is often the right choice for targeted and relatively straightforward antibody-related quantification in translational research. A personalized medicine antibody analysis strategy becomes more appropriate when the study requires deeper interpretation across patient-derived matrices, subgroup comparisons, specificity review, or multi-attribute evidence beyond a single endpoint.
The practical dividing line is this: if your team only needs a quantitative readout for a defined marker, ELISA may be sufficient. If your team needs to explain whether that signal reflects true biology, interference, binding behavior, or subgroup-specific differences, broader antibody analysis is usually the better fit. Many programs benefit from combining both.
If you are planning a biomarker, target engagement, or patient stratification study and need to decide between ELISA, an orthogonal method, or a custom workflow, contact us at the project team to discuss the project and align the assay path with your sample matrix, reporting needs, and translational decision stage.
FAQ
Is ELISA enough for personalized medicine antibody studies?
Sometimes. ELISA is often sufficient when the study asks a narrow quantitative question about a known analyte in a controlled matrix. It becomes less informative when the program also needs subgroup-level interpretation, specificity confirmation, or an explanation for conflicting signals in patient-derived samples.
What does personalized medicine antibody analysis include beyond ELISA?
It may include custom assay design, matrix-specific optimization, cross-reactivity review, specificity testing, affinity or binding characterization, and orthogonal confirmation. The exact combination should follow the decision the study needs to support rather than a fixed platform label.
When should a team add an orthogonal method after ELISA?
A team should consider it when ELISA results are decision-relevant but not self-explanatory. Common triggers include unexpected subgroup separation, disagreement with another dataset, suspected matrix interference, or a need to distinguish true target-related signal from off-target effects.
Does multiplexing automatically make ELISA the wrong choice?
No. ELISA may still be useful for a focused part of the workflow, especially when one marker needs straightforward quantification. But if the study depends on comparing multiple markers or attributes in limited sample volume, a broader analysis strategy may be a better fit than extending a single-analyte format beyond its natural use case.
How do patient-derived matrices change method selection?
They increase the chance that background proteins, endogenous antibodies, treatment-related components, or collection variability will affect readout behavior. That does not rule out ELISA, but it does increase the value of matrix-focused controls, orthogonal confirmation, and customized workflow design.
What should be defined before requesting assay development support?
Teams should clarify the analyte or target concept, sample type, cohort structure, expected concentration range if known, required output type, available sample volume, and the decision the data will support. Those inputs make it easier to judge whether a standard ELISA, a hybrid plan, or a broader custom analysis workflow is justified.
How to order?

