
Identifying Disease Biomarkers with Phage Immunoprecipitation Sequencing
Introduction
Disease biomarker discovery often fails when the signal is real but the screening strategy is too narrow. A patient cohort may contain disease-associated antibodies, yet a single-antigen assay can miss the relevant target. Autoimmune diseases, infectious disease sequelae, cancer- associated immune responses, and vaccine-related studies often involve broad and heterogeneous antibody recognition. Researchers need a way to compare antibody reactivity across many candidate antigens without assuming the correct target in advance.
Phage immunoprecipitation sequencing addresses this problem by combining phage display peptide libraries with antibody capture and next-generation sequencing. Antibody-containing samples are incubated with a library of displayed peptides. Antibodies bind peptide sequences that resemble recognized antigen regions. The antibody-bound phage particles are enriched by immunoprecipitation, sequenced, and mapped back to peptide identities. The resulting enrichment profile can reveal candidate disease biomarkers for downstream validation.
The value of phage immunoprecipitation sequencing depends on study design. Disease and control groups must be comparable. The peptide library must represent the relevant antigen space. Controls must separate disease-associated enrichment from background binding. Candidate biomarkers must be validated with orthogonal assays before they are treated as diagnostic or mechanistic evidence. For teams planning antibody biomarker discovery, MtoZ Biolabs can help evaluate whether PhIP-Seq fits the disease model, sample set, and validation goal.
Related Services
| Research Need | Recommended Service |
| Need broad antibody reactivity screening across disease and control groups | PhIP-Seq Antibody Analysis Service |
| Need peptide-level epitope discovery for candidate biomarkers | Antibody Epitope Mapping Service |
| Need targeted validation of selected peptide candidates | Peptide Array-Based Epitope Mapping Service |
| Need antibody sequence support for discovery or engineering programs | Antibody Sequencing Service |
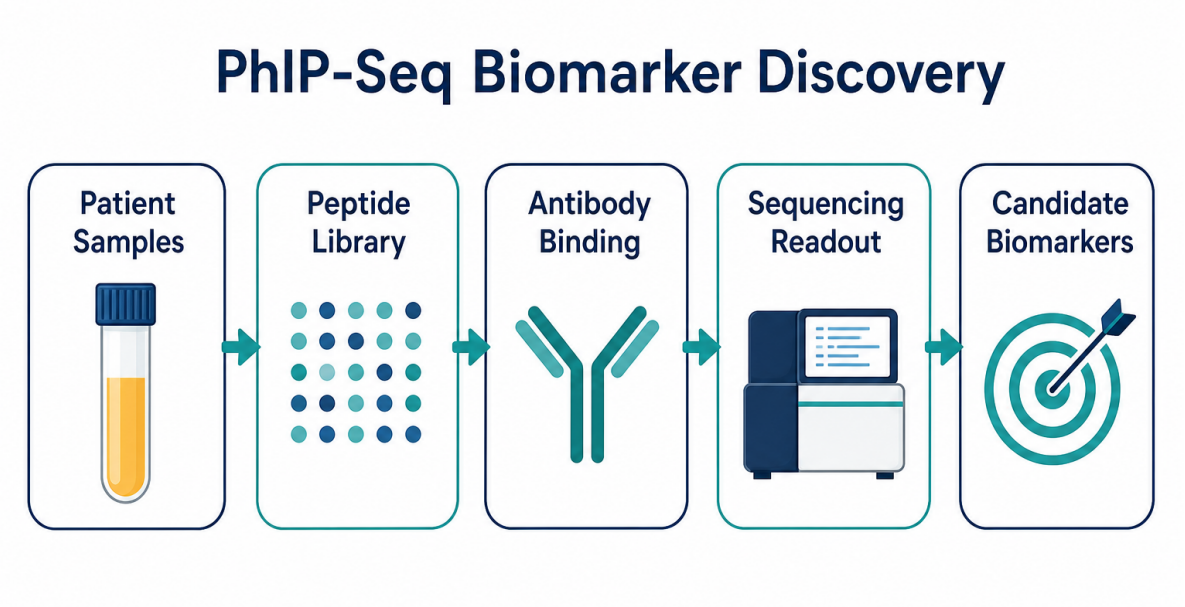
Figure 1. Phage immunoprecipitation sequencing screens antibody reactivity across peptide libraries to prioritize candidate disease biomarkers.
Why Antibody Biomarkers Are Difficult to Discover
Antibody biomarkers are attractive because antibodies can reflect immune history, disease activity, infection exposure, tumor-associated responses, or autoimmune recognition. Serum and plasma samples are also easier to collect than many tissue specimens. However, antibody signals are often complex. A disease group may include several immune subtypes. A control group may have background exposure or cross-reactive antibodies. A candidate antigen may be present only in a subset of patients.
Traditional assays are useful when the target is already known. ELISA, Western blotting, and targeted immunoassays can test specific antigens or proteins. These methods are less efficient when the target space is broad or when researchers need to discover candidate antigen regions before selecting validation assays.
Phage immunoprecipitation sequencing is useful in this discovery setting because the method can profile antibody binding across many displayed peptides in parallel. Instead of asking whether antibodies bind one selected antigen, the experiment asks which peptide features are enriched in disease-associated samples compared with controls.
How Phage Immunoprecipitation Sequencing Finds Candidate Biomarkers
The core logic is comparative enrichment. A phage display peptide library provides a searchable collection of peptide sequences. Serum, plasma, or another antibody-containing sample is exposed to the library. Antibodies bind displayed peptides that match linear epitopes or motif-like recognition patterns. Immunoprecipitation captures antibody-bound phage particles, and sequencing identifies the enriched peptide clones.
The output is usually a peptide-by-sample enrichment matrix. Each row represents a peptide or peptide region, and each column represents a sample. Statistical analysis can compare enrichment between disease and control groups, clinical subtypes, disease stages, treatment- response groups, or longitudinal time points.
A candidate disease biomarker is not just a peptide with a high read count. A stronger candidate shows enrichment above background, reproducibility across replicates, association with a defined disease group, biological plausibility, and support from neighboring peptides or related antigen regions. In well-designed studies, PhIP-Seq narrows a broad antigen space into a smaller candidate list for targeted validation.
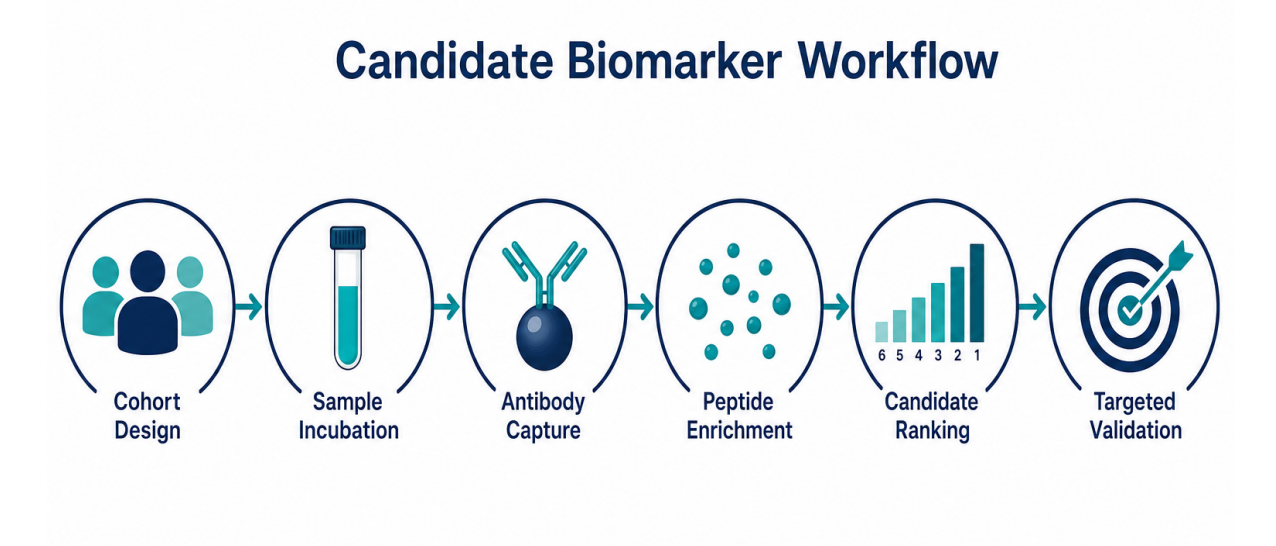
Figure 2. Candidate biomarker discovery moves from cohort samples to peptide enrichment, statistical comparison, prioritization, and validation.
Selecting the Right Disease Cohort
Cohort design is one of the strongest predictors of biomarker quality. A disease biomarker should distinguish a clinically meaningful group from an appropriate comparison group. The comparison may be disease versus healthy control, early-stage versus late-stage disease, responder versus non-responder, pre-treatment versus post-treatment, or infection-exposed versus unexposed.
Controls should match the study question. Healthy controls may be useful in early discovery, but disease controls may be more relevant when the final goal is differential diagnosis. For autoimmune studies, controls should consider age, sex, inflammatory background, medication status, and related disease conditions. For infectious disease studies, controls should consider exposure history, vaccination status, geography, and sampling time.
Metadata quality also matters. Clinical status, sample collection date, treatment history, disease severity, storage condition, and freeze-thaw history can all affect interpretation. A peptide signal may look disease-associated if one group was collected or stored differently. A balanced processing plan reduces this risk.
Matching the Peptide Library to the Biomarker Question
The peptide library defines what phage immunoprecipitation sequencing can detect. A human proteome library can support autoantibody biomarker discovery. A pathogen-derived library can support infection-associated biomarker studies. A tumor antigen library can explore cancer- related immune recognition. A custom tiled library can focus on proteins, variants, or antigen families linked to a hypothesis.
The broadest library is not always the best choice. A very large library can increase discovery potential, but it also increases multiple testing burden, data complexity, and background interpretation. A focused library can produce cleaner results when the disease mechanism or antigen family is already known.
Library design should consider peptide length, tiling density, overlap, sequence redundancy, clone representation, and antigen coverage. Because phage display peptide libraries are strongest for linear epitopes and motif-like recognition, results should be interpreted carefully when disease antibodies are expected to recognize conformational or post-translationally modified epitopes.
Controlling Background and False Positives
Biomarker discovery needs strict background control. Some peptides may bind nonspecifically to beads, capture reagents, serum components, or phage particles. Some sequences may appear enriched because of library imbalance or amplification bias. Some antibody signals may reflect common exposure rather than disease-specific biology.
A useful PhIP-Seq biomarker study includes input library sequencing, no-serum controls, technical replicates, biological controls, and batch-aware analysis. Negative controls help define background enrichment. Replicates help identify unstable signals. Input sequencing helps distinguish true antibody enrichment from starting library abundance.
Candidate filtering should be conservative. Researchers should evaluate fold enrichment, statistical significance, background behavior, replicate agreement, neighboring peptide support, and group-level consistency. A ranked peptide list should not be treated as a final biomarker panel without validation.
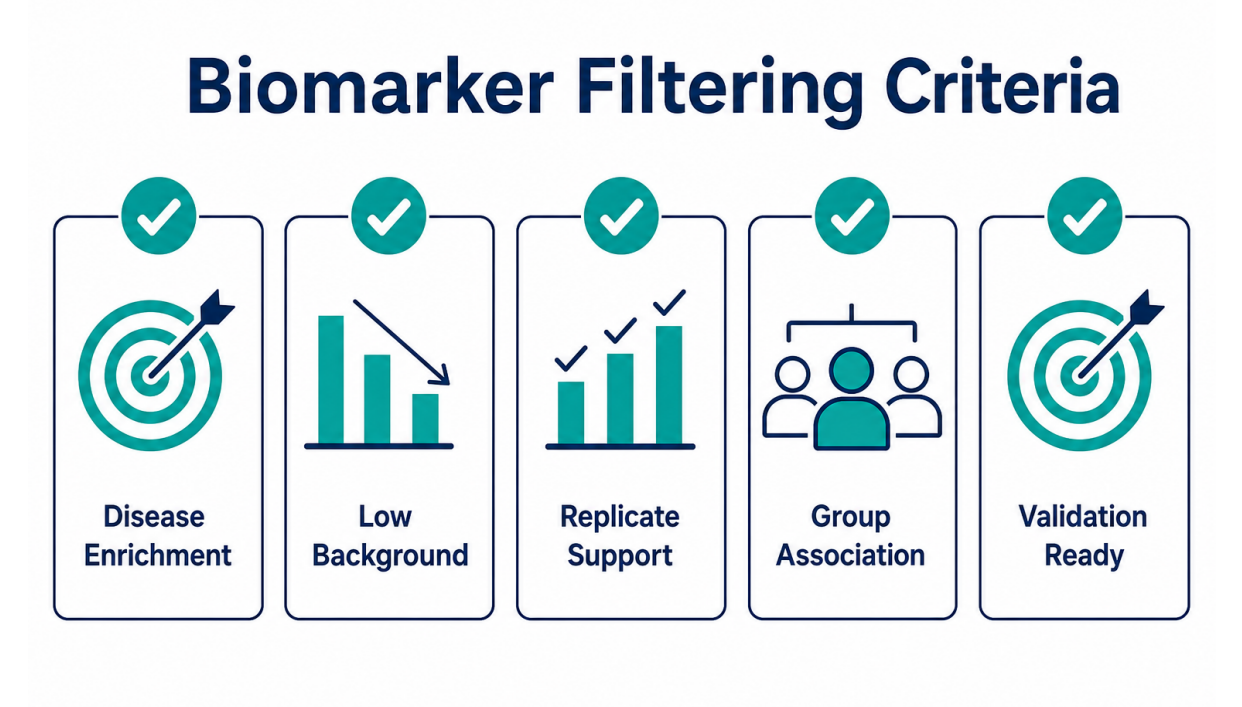
Figure 3. Candidate biomarkers should pass enrichment, reproducibility, background, group association, and validation-readiness filters.
Prioritizing Candidate Disease Biomarkers
After enrichment analysis, researchers often face a long candidate list. Prioritization turns this list into a practical validation plan. A useful candidate should answer a specific disease question. Does the peptide distinguish disease from controls? Does the signal appear in early-stage samples? Does the signal correlate with severity, treatment response, or clinical subtype? Does the antigen have plausible disease relevance?
Neighboring peptide support can improve confidence. If multiple overlapping peptides from the same region are enriched, the result may indicate a candidate epitope region rather than a single isolated hit. Protein-level aggregation can also help when several peptides from the same antigen show consistent disease-group enrichment.
Candidate selection should balance statistical strength and biological relevance. The top statistical hit is not always the best validation target if the signal is driven by a few samples or a poorly annotated region. A moderate but reproducible signal across a clinically meaningful subgroup may be more valuable.
Validation Strategy for Biomarker Discovery
Validation should be planned before discovery data are generated. PhIP-Seq is a screening and prioritization method. Candidate peptides need confirmation with independent assays and, when possible, independent sample cohorts.
Peptide arrays can test selected peptide regions across larger cohorts. ELISA can support targeted measurement when the antigen or peptide format is suitable. Western blotting can provide protein-level context for selected targets. Targeted immunoassays can evaluate candidate panels. Protein-based binding assays may be needed when native structure matters.
Validation should test performance, not just presence. Researchers may evaluate sensitivity, specificity, receiver operating characteristic behavior, positive and negative predictive value, subgroup performance, and reproducibility across cohorts. Early discovery does not need to answer every clinical performance question, but the validation plan should match the intended use.
When PhIP-Seq Is a Good Fit for Biomarker Studies
PhIP-Seq is a good fit when researchers need broad antibody profiling and the likely biomarker may be peptide-based or epitope-related. The method is especially useful when the disease target is unknown, when multiple antigen candidates are plausible, or when cohort comparison is central to the question.
The approach can be useful for autoimmune biomarker discovery, infection-associated serological signatures, vaccine response stratification, cancer immune-response studies, and exploratory disease subgroup analysis. The method can also help identify candidate peptide regions for later assay development.
PhIP-Seq may be less suitable when the final biomarker is expected to depend on a conformational epitope, glycan structure, lipid antigen, or native protein complex that cannot be represented by linear peptides. In these cases, researchers should evaluate whether PhIP-Seq should be paired with peptide arrays, protein assays, structural methods, or other validation workflows.
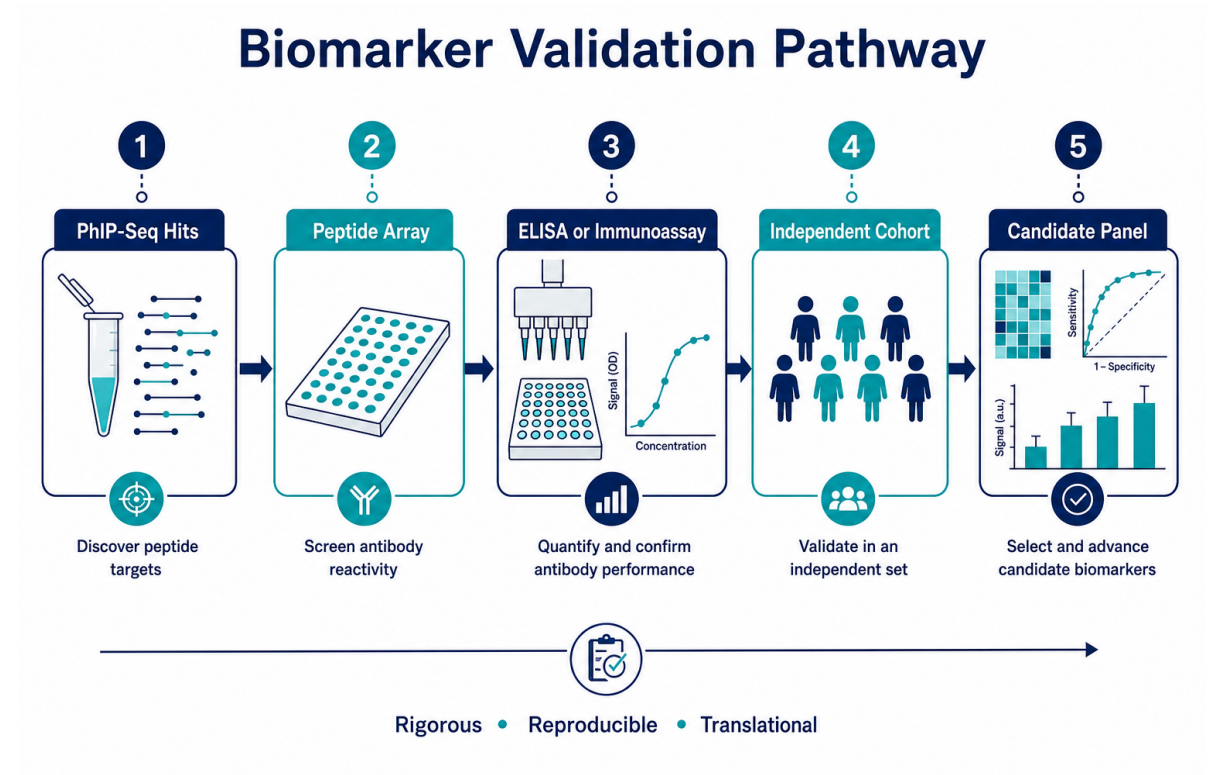
Figure 4. PhIP-Seq biomarker discovery should connect screening results to targeted validation and independent cohort testing.
What a Biomarker-Focused Report Should Include
A biomarker-focused report should make the evidence chain transparent. The report should describe the peptide library, sample groups, controls, sequencing metrics, read mapping, enrichment method, statistical comparison, candidate ranking, and QC results.
The report should also explain why each candidate was prioritized. Useful evidence includes disease-group enrichment, replicate agreement, background filtering, peptide region support, antigen annotation, subgroup association, and recommended validation methods. A report that only provides a ranked table leaves too much interpretation to the researcher.
For publication-oriented or translational projects, the report should separate discovery findings from validated conclusions. MtoZ Biolabs supports PhIP-Seq biomarker projects by helping researchers connect antibody profiling data with candidate prioritization, validation planning, and follow-up assay selection.
Frequently Asked Questions
1. Can PhIP-Seq discover disease biomarkers?
Yes. PhIP-Seq can identify candidate antibody-reactive peptides that differ between disease and control groups. The results should be treated as discovery candidates until validated in independent assays or cohorts.
2. What sample types are commonly used for PhIP-Seq biomarker discovery?
Serum and plasma are commonly used because they contain circulating antibodies. Other antibody-containing fluids may be considered if sample quality, antibody abundance, and disease relevance support the study design.
3. How are PhIP-Seq biomarker candidates validated?
Candidate peptides may be validated with peptide arrays, ELISA, Western blotting, targeted immunoassays, or protein-based binding assays. Independent cohorts are important when the goal is biomarker development.
4. Can PhIP-Seq distinguish disease subtypes?
PhIP-Seq can support disease subtype analysis when the cohort is designed for that comparison. Subtype discovery requires enough samples, clear clinical labels, balanced processing, and appropriate statistical analysis.
5. Does a high enrichment score mean a peptide is a biomarker?
No. High enrichment is only one piece of evidence. A candidate biomarker should also show background control, replicate consistency, group association, biological plausibility, and validation support.
Conclusion
Phage immunoprecipitation sequencing can help researchers identify disease biomarker candidates by profiling antibody reactivity across broad peptide libraries. The method is most valuable when the antigen target is unknown, the disease signal may be heterogeneous, and the study requires comparison across well-defined sample groups.
Successful biomarker discovery depends on more than sequencing output. Cohort design, library selection, background control, candidate prioritization, and validation planning determine whether enriched peptides become useful research leads. To evaluate whether PhIP-Seq biomarker discovery fits your disease model and sample set, contact MtoZ Biolabs for technical guidance before launching a full screening study.
How to order?

