
Applications of Bottom-Up Proteomics in Clinical Research: Biomarkers, Subtyping, and Translational Workflows
-
Bottom-up proteomics fits diverse clinical matrices when sample prep addresses abundance bias.
-
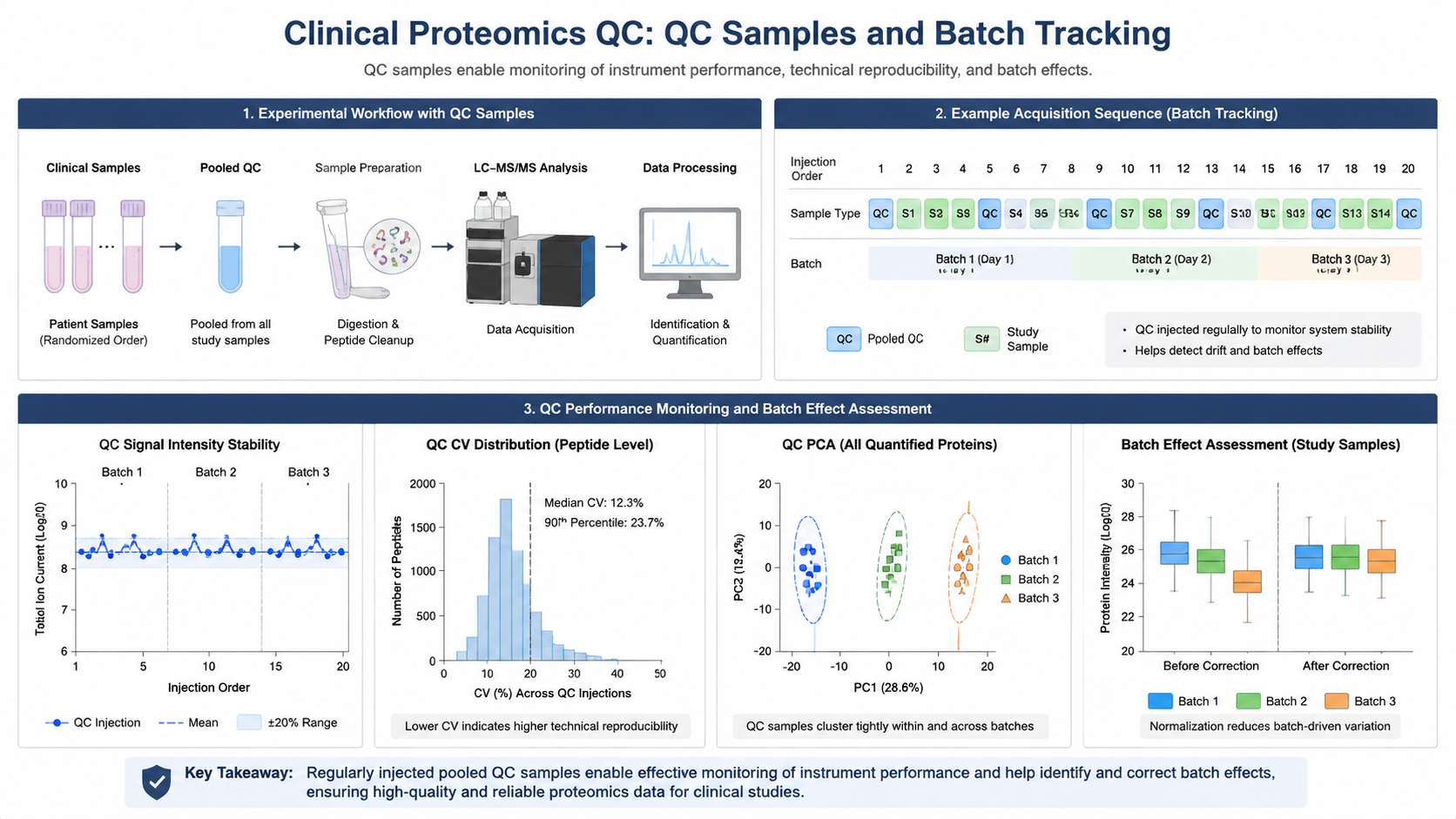
Biomarker programs need cohort design, depletion or fractionation, and strict batch QC.
-
TMT, SILAC, and label-free quantification integrate with multi-omics when planned early.
-
PTM layers add signaling context to drug studies.
-
Reproducibility depends on reference standards and tracked preparation workflows.
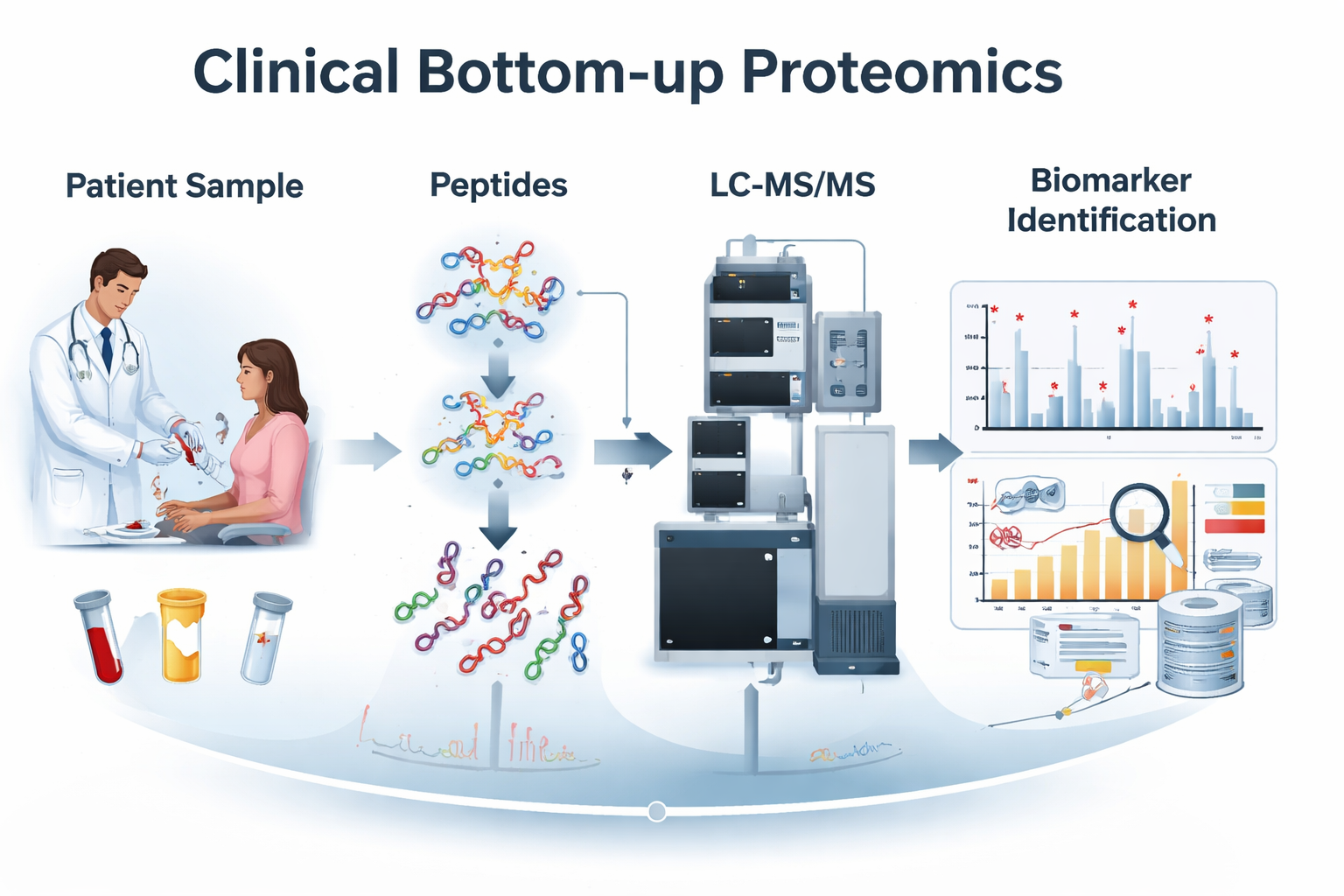
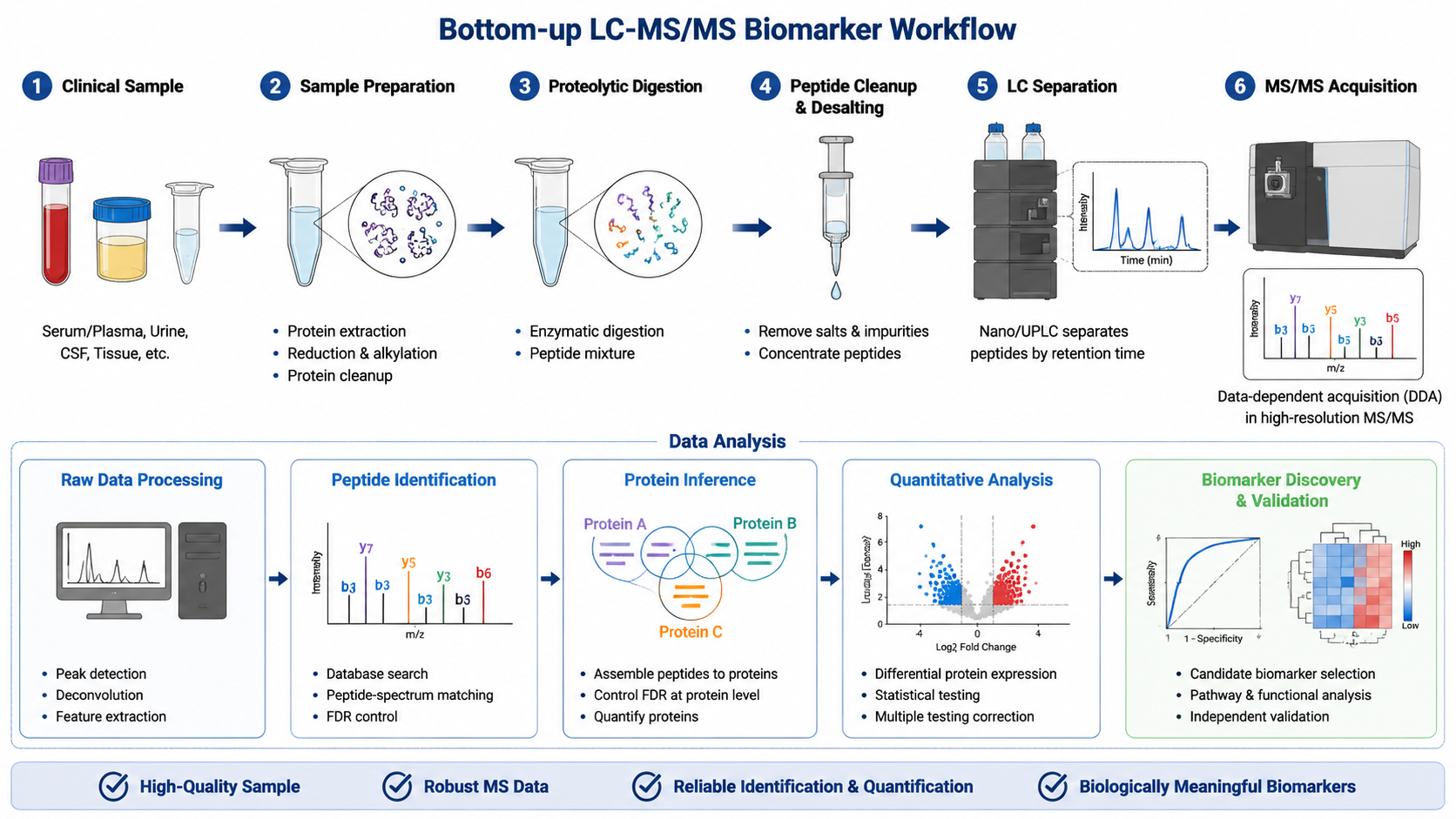
Bottom-up proteomics digests proteins to peptides for LC-MS/MS identification and quantification. In clinical research, that workflow scales to plasma, urine, tissue, and CSF while supporting biomarker discovery, molecular subtyping, and drug-response studies.
Key Takeaways
What Is Bottom-Up Proteomics?
Proteins are enzymatically cleaved to peptides, then analyzed by high-resolution MS. Bottom-up handles complex clinical proteomes with established pipelines and higher throughput for large patient sets.
Related Services
Clinical Proteomics Research Solutions
Top Down and Bottom Up Proteomics Service
Bottom-Up MS-Based PTM Analysis Service
Key Clinical Applications
1. Biomarker Discovery
Compare disease versus control proteomes for diagnostic, prognostic, or response markers across oncology, autoimmunity, neurodegeneration, and cardiovascular research.
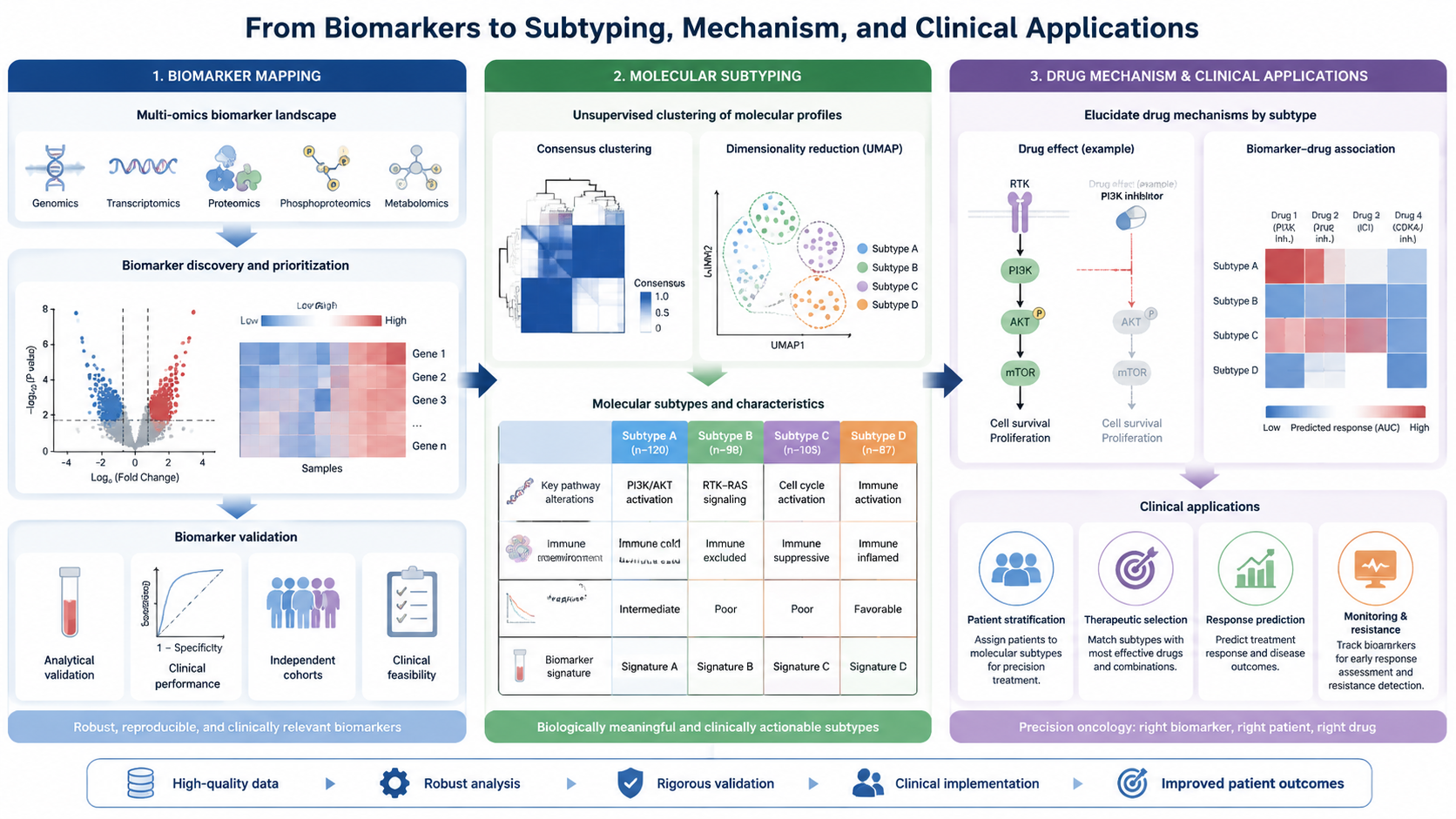
2. Disease Subtyping and Precision Medicine
Protein signatures separate molecular subtypes and can support machine-learning classifiers with adequate cohort size and QC.
3. Drug Targets and Mechanism Studies
Measure network shifts after treatment; add PTM proteomics when pathway regulation is central.
Clinical Sample Challenges
| Challenge | Impact | Mitigation |
|---|---|---|
| High dynamic range | Masked low-abundance signals | Depletion, fractionation, deep MS |
| Cohort heterogeneity | Noisy comparisons | Power planning; balanced batches |
| Batch effects | False biomarkers | QC pools; randomized run order |
FAQ
1. Why bottom-up over top-down in clinical cohorts?
Higher throughput and mature pipelines for large heterogeneous sample sets.
2. Which clinical samples are compatible?
Plasma, serum, urine, tissues, and CSF when prep matches matrix complexity.
Conclusion
Bottom-up proteomics supports clinical translation when matrix complexity, quantification, and QC are built into the study design from the start.
How to order?

